I’m still waiting to hear back from the surgeon. I read the notes. It sounds like the surgery was pretty intense.
The TME included cutting anterior to the Denonvellier’s fascia, which sounds like anything more would be a prostatectomy.
His surgeon operated to the MRF and handed control over to the urologist who operated past the MRF into the DVF.
The surgeons felt confident that all the cancer was removed.
I unfortunately had to get all the feedback from DH who told me the margin was not clear. But he also told me the surgeons sounded very optimistic, although there was discussion about post op radiation which is concerning.
The urologist feedback to DH was optimistic and that his prostate did not need to be removed.
So I feel like we are in some sort of gray area where maybe the prostatectomy might or might not be forthcoming, but could be avoided at this particular time. Which is good for a couple reasons because recovering from an APR and a prostatectomy simultaneously sounds daunting. Of course the other reason is perhaps prostatectomy may never be needed at all.
So I will know more after she returns my call.
DH is recovering surprisingly well!
Need advice: Margins were not clear
Re: Need advice: Margins were not clear
DH 61
2019 4A t3 n2 m1a
8/23 C-scopy, 5+cm mass. CEA:4.1
9/16 MSS. MRI: 2 lvr mets: 2.7 & 7mm
9/30 Start FOLFOX 1-6
10/4 Lg lvr met ~3.7cm, pri tmr stable.
CEA: 10/13,12.5;10/27-12/8 btw 4.7 & 3.1
11/5 both lvr mets ~ 2/3 smaller.
12/17 PET: significant improv.
2020
MWA 2/5, Lap resection 2/11
CEA: 3/1-5/31 btw 2.1&2.9
3/2 start FOLFOX 7-12
7/23-29 EBRT
10/2/2020 NED/W&W
4/2022 EUS-FNA,MRI: recur.;
5/2022:CT scan no mets. APR.
7-12/2023 Xeloda
4/2023 CT/MRI NED
2019 4A t3 n2 m1a
8/23 C-scopy, 5+cm mass. CEA:4.1
9/16 MSS. MRI: 2 lvr mets: 2.7 & 7mm
9/30 Start FOLFOX 1-6
10/4 Lg lvr met ~3.7cm, pri tmr stable.
CEA: 10/13,12.5;10/27-12/8 btw 4.7 & 3.1
11/5 both lvr mets ~ 2/3 smaller.
12/17 PET: significant improv.
2020
MWA 2/5, Lap resection 2/11
CEA: 3/1-5/31 btw 2.1&2.9
3/2 start FOLFOX 7-12
7/23-29 EBRT
10/2/2020 NED/W&W
4/2022 EUS-FNA,MRI: recur.;
5/2022:CT scan no mets. APR.
7-12/2023 Xeloda
4/2023 CT/MRI NED

Re: Need advice: Margins were not clear
jsbsf wrote:... I unfortunately had to get all the feedback from DH who told me the margin was not clear. But he also told me the surgeons sounded very optimistic, although there was discussion about post op radiation which is concerning....
jsbsf -
Your DH's situation seems very complicated, and I can understand why you would want to have a number of second opinions and to receive other viewpoints for comparison before making a decision on radiation vs. chemotherapy.
I have some thoughts on this issue that might be of interest to you, but on the other hand they might not be very relevant since my situation was very different since it was an emergency open surgery for a T4b tumor followed by 5 weeks of chemo/radiation and then a subsequent XELOX adjuvant therapy regimen, while your DH's situation was a t3 tumor treated under a W&W protocol leading eventually to the recent robotic APR surgery, with a possibility now for adjuvant therapy, either chemo/radiation or FOLFOX. Even though our two scenarios are very different, there still might be some points worthwhile discussing.
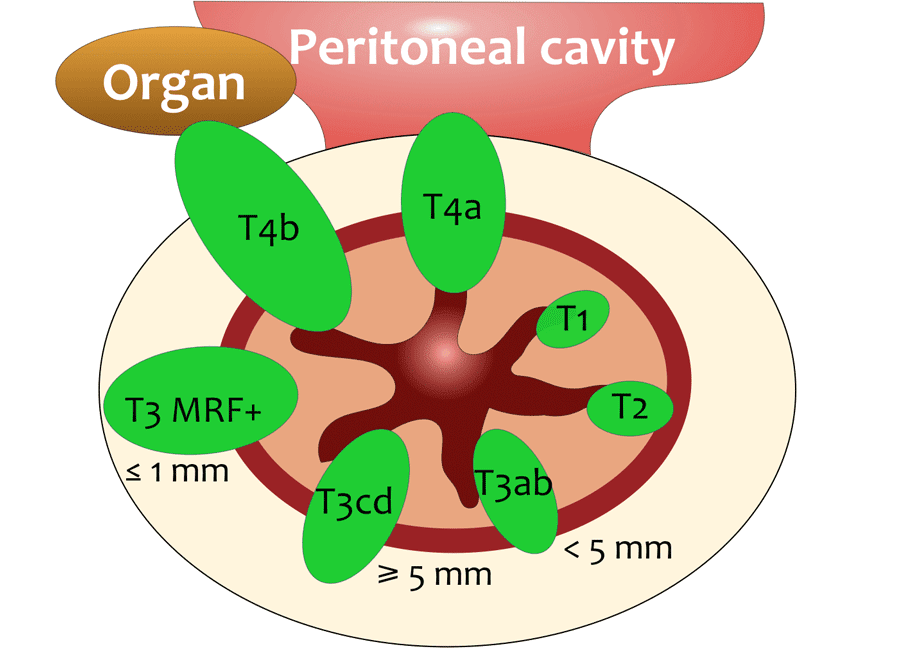
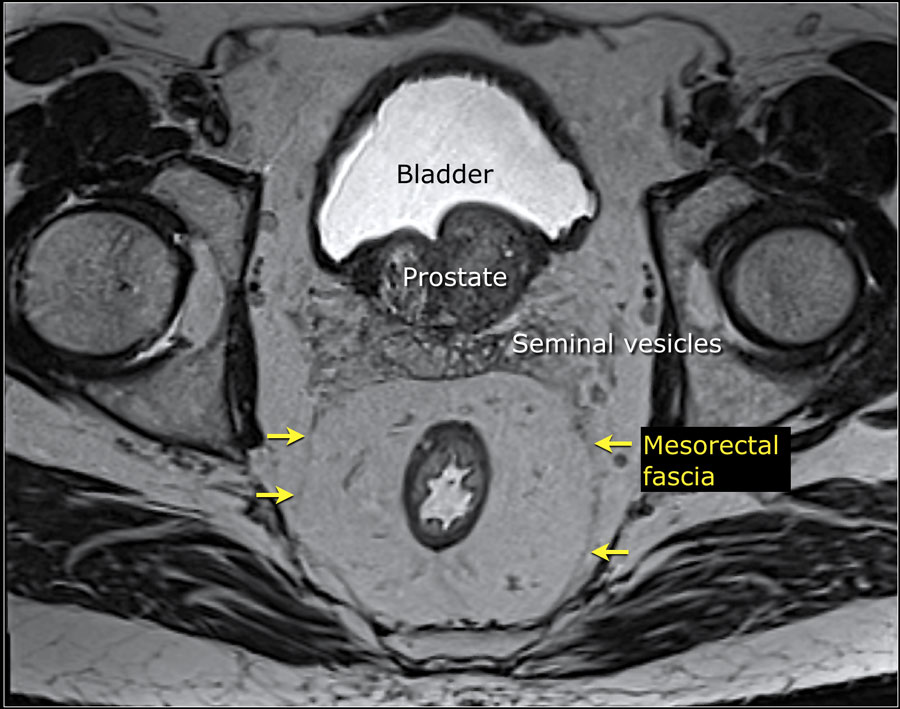
Visually, our two scenarios can be viewed here: My tumor was a T4b tumor invading the left seminal vesicle, while DH's tumor was a T3 tumor breaching the Meso Rectal Fascia , i.e., T3 MRF+
In spite of these differences, I will try to make some relevant comments.
Here are some of my concerns:
- Adjuvant radiation therapy - targeted how and where?
Your surgeon seems to be in favor of radiation for dealing with cancer cells possibly left behind by surgery. But this surgery was an Abdominal Perineal Resection (APR) that involved removing the whole rectum plus the anal canal, and probably the recto-sigmoid junction as well. The specimen sent to pathology must have been a fairly long one -- maybe half a foot long or longer, but where along the edge of this lengthy specimen did the pathologist find the positive-margin cancer cells? Was it down near the sphincter, or up near the recto-sigmoid junction, or somewhere in the middle? Does the pathology report state specifically where the anatomical site was where the cancer cells were found, or is it just the surgeon's guess? If the current hypothesis is that the cells are near the prostate, then how can the pathologist know for sure that the cancer cells found at the margin were actually near the prostate if the prostate itself was not included as part of the specimen? So, my concern is how are they going to know exactly where to target the radiation when it comes time to set up the machine, or are they just going to be using a shotgun approach like shooting in the dark? - Specific type of EBRT?
There is another issue that I think should be addressed. It is to determine the exact type of EBRT that was done in July 2020, as well as the type of EBRT proposed for adjuvant therapy now. It appears that the July 2020 EBRT was a 5 day, high intensity, chemo/radiation short course, probably targeting the rectal tumor and adjacent lymph nodes. But what is it now that is being proposed for adjuvant therapy, and which of the available EBRT machines/protocols will be used? There are several types of EBRT available, all depending on the specific machine models used and their capabilities for targeted or modulated radiation:
https://radonc.ucsf.edu/conditions-treatments/types-of-treatment/external-beam-radiation-therapy-ebrt/
There are some questions that need to be asked right now, in my opinion. What kind of machine will be used? What capability does it have for targeting the radiation in specific locations? How much radiation will be delivered in total, and for how many days altogether? Where, exactly, will the radiation beams be focused, and what evidence do they have that it will be these particular regions that need to be targeted?
- Organs shifting location after APR surgery?
There is another issue that might be relevant, but I can't say for sure since I don't know that much about anatomy. It is to ask which organs or structures are now located where the rectum and anal canal used to be? Have some organs moved position to fill in the gap produced by the APR surgery? For example, has part of the small bowel moved over to this area to fill in the gap? Some organs or structures are pretty much fixed in location and would not shift around, like the kidneys, bladder, and prostate, for example, but others might gravitate toward the void caused by the APR. This might be relevant when they start programming the targeted radiation. For example, a loop of the small intestine might be located now where the rectum used to be, or a vital nerve sheath coming from the spinal cord might have been pushed over into this area. There might be some organs or anatomical structures now pressing against the prostate but which should never be exposed to excessive radiation. I would want to know what kind of experience the radiation oncologists have had in targeting radiation into uncharted territory caused by an APR surgery. How many successful post-APR adjuvant radiation therapy interventions have they actually done in the past? - Prostatectomy after double courses of radiation?
Apparently DH has talked to the urologist who was on standby for the APR surgery, but has he ever had an actual consultation with a urologist to go over the pro's and con's of a post-radiation prostatectomy? It might be worthwhile to have both a first-opinion consultation as well as a second opinion on this issue. I'm pretty sure that my urologist would never perform a prostatectomy on a patient who had had two regimens of pelvic radiation therapy. It's far too risky, in my opinion.
{kind=link}
Re: Need advice: Margins were not clear
In March of 2019 I had a partial cystectomy for rectal cancer involvement in the bladder. One of the margins came back positive but the surgeon insisted he got it all. 2 years later it was back with a spot in the peritoneum also. At Memorial Sloan Kettering they initially didn't even want to operate but proceeded with an operation after discussing it at tumor board October 2021. I had chemo 3 months prior to the operation and 3 months after. I agree with getting evaluated at a major cancer center.
46 rectal ca. 12/16
LAR 1/17, 0/30 nodes +
CT 6/18 - 4 nodules R lung + 3 spots in left lung (largest 1.7cm)
Laser pulm. metastectomy B Germany 10/18 and 11/18
12/18 blood in urine -> rectal ca met on bladder
3/19 partial cystectomy
4/19 MSK self referral
Avastin + 5fu x 6 mos
3/21 blood in urine ->bladder recurrence + R ext iliac node
10/21 MSK partial cystectomy node turned out to be peritoneal implant
12/22 UCSD CRS surgery PCI score 8, 1m small bowel resected
NED after 6 and 1/2 years
LAR 1/17, 0/30 nodes +
CT 6/18 - 4 nodules R lung + 3 spots in left lung (largest 1.7cm)
Laser pulm. metastectomy B Germany 10/18 and 11/18
12/18 blood in urine -> rectal ca met on bladder
3/19 partial cystectomy
4/19 MSK self referral
Avastin + 5fu x 6 mos
3/21 blood in urine ->bladder recurrence + R ext iliac node
10/21 MSK partial cystectomy node turned out to be peritoneal implant
12/22 UCSD CRS surgery PCI score 8, 1m small bowel resected
NED after 6 and 1/2 years
Re: Need advice: Margins were not clear
DH’s primary tumor was destroyed with chemo followed up by EBRT. The result was an area of soft tissue that had eventually been determined to have cancer cells. The cancer cells were not like the original tumor in that there was no vascular invasion. In fact the ultrasound couldn’t really pick up a tumor. The MRI could detect that the “mass” extended to the prostate, but MRIs can’t determine if cells are cancerous. The MRI was not certain if the mass invaded the prostate, but the ultrasound stated that the prostate was not involved. The MRI considered it t3c and MRF+. Several biopsies were taken in which cancer was found in a FNA, which led to the decision to move forward with the APR.
His liver was also visually examined prior to the APR. No metastases we’re observed.
The pathology reported no positive lymph nodes, but a positive margin. It is my understanding that the positive margin was CRM, and that the other (non radial) margins were clear since the APR removed pretty much everything.
His surgery went all the way to the seminal vesicles. Colorectal surgeon operated to the MRF, and the urologist took over and examined the prostate, and concluded a biopsy was not necessary based on a visual examination. He removed tissue up to the seminal vesicles, and enough that it is actually considered more likely to cause nerve damage. In fact they were worried he’d need a catheter for an extended period. Luckily that was not the case.
So, although the cancer cells were found in the margin, they feel that any cancerous cells that would remain are in a very narrow amount of fat tissue which is outside the prostate. Additionally the urologist felt that the high amount of heat used (I guess the robotic surgery additionally cauterizes the wound) would likely kill cells in the immediate area.
My understanding is that the entire area that was previously radiated was removed.
The urologist explained that if radiation is determined to be administered, that it would not be EBRT, but something milder that would be applied along that plane. I didn’t get the name for the type of radiation he was referring to. But everything still needs to be reviewed by the team, and we probably won’t get a recommendation until close to the end of June.
The surgeon seemed to feel like the outcome of the surgery was great, so much that she believes no adjuvant therapy may even be the best approach, but we still need to hear from his oncologist. Her optimism makes me hopeful. It’s a multidisciplinary team of board certified surgeons along with his oncologist, and they will debate…
DH and I are partial to chemo since it worked so well initially. But of course we can only ask for that and see what happens. Also, I feel that in his case, the chance of systematic recurrence is greater than that of local recurrence, even with the positive margin. But a lot of weight is given to all negative lymph nodes.
His liver was also visually examined prior to the APR. No metastases we’re observed.
The pathology reported no positive lymph nodes, but a positive margin. It is my understanding that the positive margin was CRM, and that the other (non radial) margins were clear since the APR removed pretty much everything.
His surgery went all the way to the seminal vesicles. Colorectal surgeon operated to the MRF, and the urologist took over and examined the prostate, and concluded a biopsy was not necessary based on a visual examination. He removed tissue up to the seminal vesicles, and enough that it is actually considered more likely to cause nerve damage. In fact they were worried he’d need a catheter for an extended period. Luckily that was not the case.
So, although the cancer cells were found in the margin, they feel that any cancerous cells that would remain are in a very narrow amount of fat tissue which is outside the prostate. Additionally the urologist felt that the high amount of heat used (I guess the robotic surgery additionally cauterizes the wound) would likely kill cells in the immediate area.
My understanding is that the entire area that was previously radiated was removed.
The urologist explained that if radiation is determined to be administered, that it would not be EBRT, but something milder that would be applied along that plane. I didn’t get the name for the type of radiation he was referring to. But everything still needs to be reviewed by the team, and we probably won’t get a recommendation until close to the end of June.
The surgeon seemed to feel like the outcome of the surgery was great, so much that she believes no adjuvant therapy may even be the best approach, but we still need to hear from his oncologist. Her optimism makes me hopeful. It’s a multidisciplinary team of board certified surgeons along with his oncologist, and they will debate…
DH and I are partial to chemo since it worked so well initially. But of course we can only ask for that and see what happens. Also, I feel that in his case, the chance of systematic recurrence is greater than that of local recurrence, even with the positive margin. But a lot of weight is given to all negative lymph nodes.
DH 61
2019 4A t3 n2 m1a
8/23 C-scopy, 5+cm mass. CEA:4.1
9/16 MSS. MRI: 2 lvr mets: 2.7 & 7mm
9/30 Start FOLFOX 1-6
10/4 Lg lvr met ~3.7cm, pri tmr stable.
CEA: 10/13,12.5;10/27-12/8 btw 4.7 & 3.1
11/5 both lvr mets ~ 2/3 smaller.
12/17 PET: significant improv.
2020
MWA 2/5, Lap resection 2/11
CEA: 3/1-5/31 btw 2.1&2.9
3/2 start FOLFOX 7-12
7/23-29 EBRT
10/2/2020 NED/W&W
4/2022 EUS-FNA,MRI: recur.;
5/2022:CT scan no mets. APR.
7-12/2023 Xeloda
4/2023 CT/MRI NED
2019 4A t3 n2 m1a
8/23 C-scopy, 5+cm mass. CEA:4.1
9/16 MSS. MRI: 2 lvr mets: 2.7 & 7mm
9/30 Start FOLFOX 1-6
10/4 Lg lvr met ~3.7cm, pri tmr stable.
CEA: 10/13,12.5;10/27-12/8 btw 4.7 & 3.1
11/5 both lvr mets ~ 2/3 smaller.
12/17 PET: significant improv.
2020
MWA 2/5, Lap resection 2/11
CEA: 3/1-5/31 btw 2.1&2.9
3/2 start FOLFOX 7-12
7/23-29 EBRT
10/2/2020 NED/W&W
4/2022 EUS-FNA,MRI: recur.;
5/2022:CT scan no mets. APR.
7-12/2023 Xeloda
4/2023 CT/MRI NED
Re: Need advice: Margins were not clear
The board met and the oncologist called today with his recommendation. Everyone wanted to stand by and monitor since they all feel quite optimistic. He dissented, and opted for “insurance”.
I hadn’t heard back from the oncologist for the second opinion which I requested over 3 weeks ago, and wanted to follow up after hearing back from ours. Incidentally, ours asked DH if he knows Dr A. DH vaguely remembered her name, however I know exactly who she is since she was my second opinion. Apparently, she already reached out to him and they discussed his case among themselves.
So I feel pretty confident as she is excellent.
DH was offered 3 months of adjuvant Xeloda, which he should start in a couple weeks. Even though they feel his cancer won’t return, this should seal the deal.
I hadn’t heard back from the oncologist for the second opinion which I requested over 3 weeks ago, and wanted to follow up after hearing back from ours. Incidentally, ours asked DH if he knows Dr A. DH vaguely remembered her name, however I know exactly who she is since she was my second opinion. Apparently, she already reached out to him and they discussed his case among themselves.
So I feel pretty confident as she is excellent.
DH was offered 3 months of adjuvant Xeloda, which he should start in a couple weeks. Even though they feel his cancer won’t return, this should seal the deal.
DH 61
2019 4A t3 n2 m1a
8/23 C-scopy, 5+cm mass. CEA:4.1
9/16 MSS. MRI: 2 lvr mets: 2.7 & 7mm
9/30 Start FOLFOX 1-6
10/4 Lg lvr met ~3.7cm, pri tmr stable.
CEA: 10/13,12.5;10/27-12/8 btw 4.7 & 3.1
11/5 both lvr mets ~ 2/3 smaller.
12/17 PET: significant improv.
2020
MWA 2/5, Lap resection 2/11
CEA: 3/1-5/31 btw 2.1&2.9
3/2 start FOLFOX 7-12
7/23-29 EBRT
10/2/2020 NED/W&W
4/2022 EUS-FNA,MRI: recur.;
5/2022:CT scan no mets. APR.
7-12/2023 Xeloda
4/2023 CT/MRI NED
2019 4A t3 n2 m1a
8/23 C-scopy, 5+cm mass. CEA:4.1
9/16 MSS. MRI: 2 lvr mets: 2.7 & 7mm
9/30 Start FOLFOX 1-6
10/4 Lg lvr met ~3.7cm, pri tmr stable.
CEA: 10/13,12.5;10/27-12/8 btw 4.7 & 3.1
11/5 both lvr mets ~ 2/3 smaller.
12/17 PET: significant improv.
2020
MWA 2/5, Lap resection 2/11
CEA: 3/1-5/31 btw 2.1&2.9
3/2 start FOLFOX 7-12
7/23-29 EBRT
10/2/2020 NED/W&W
4/2022 EUS-FNA,MRI: recur.;
5/2022:CT scan no mets. APR.
7-12/2023 Xeloda
4/2023 CT/MRI NED
Management of Xeloda (capecitabine) side effects
jsbsf wrote:The board met and the oncologist called today with his recommendation. Everyone wanted to stand by and monitor since they all feel quite optimistic. He dissented, and opted for “insurance”.
...
DH was offered 3 months of adjuvant Xeloda, which he should start in a couple weeks. Even though they feel his cancer won’t return, this should seal the deal.
jsbsf wrote:I mentioned that our oncologist recommended 3 months of Xeloda. But yesterday the pharmacist called and said it’s 6 months. 1500mg for breakfast and another 1500 for dinner 2 weeks on one week off for 8 cycles. It does seem like quite a bit for “insurance”… We are taking the chemo though, mainly because he tolerated FOLFOX pretty well the first go around.
jsbsf -
Good luck on DH's upcoming Xeloda regimen! There are a couple of things I would like to mention, however. Six months on Xeloda might not be as smooth sailing as you expect...
Xeloda is somewhat different from FOLFOX both in terms of side-effects and in how it works. Unlike FOLFOX, Xeloda (capecitabine) is a pro-drug and it must be metabolized in the digestive system in order to produce 5FU at the cellular level. This has several implications, both for how the drug is administered and how the side-effects unfold.
In terms of administration, it is very important to take the pills shortly after having the morning or evening meal. You can't take Xeloda on an empty stomach if you want it to work. Furthermore, if you have had nausea to such an extent that you vomited up your meal, then you may not have enough food in your system for the metabolism mechanism to work. Also, if you vomit up the Xeloda pills, of course this will be a problem, because the pills need to be in your system long enough for the 5FU metabolism cycle to work.
Then there is the diarrhea problem. Diarrhea is one of the main side effects of Xeloda, and it needs to be monitored very closely. This may be a bit of a problem for DH since he no longer has a rectum and diarrhea has to somehow be defined in terms of frequency of emptying the colostomy stoma bag. DH must then be told by the oncologist about how to recognize a qualifying diarrhea episode and how to count how many qualifying diarrhea episodes have occurred on a given day, since an " Increase of >=7 stools per day over baseline" is the official definition of Grade 3(Serious) diarrhea and this is what will suspend the Xeloda treatment regimen until further notice. But the thing to really worry about is the possibility of escalation of diarrhea to Grade 4 (Life-threatening), because if this ever happens, then the patient will be taken off Xeloda forever and will not be able to complete the expected 3-month or 6-month regimen. (This has happened to several people on this board already. It's not just a theoretical possibility.)
Here are the details for the special case of diarrhea. In this case, an increase of more than 6 watery stools per day is considered serious and requires immediate doctor intervention to avoid termination of treatment. This is because severe diarrhea causes excessive loss of fluids and loss of electrolytes, leading to multiple problems like kidney damage, kidney and bladder stones, etc. It should be noted that chemo-related diarrhea is different from the common traveler's diarrhea that we are familiar with. Chemo-related diarrhea is more difficult to deal with and may require special measures in order to control it. Similarly for mouth sores. These sores are not the same as the canker sores that we have had in the past. They are much more virulent and will not just go away with the passage of time. They need to be treated properly with appropriate medical procedures. If not, the mouth sores will soon gravitate to throat sores, then to larynx sores, and finally to sores in the lungs (i.e., pneumonia). Simple mouth sores need to be taken very seriously as soon as they appear, otherwise they can soon escalate out of control if they are not treated appropriately.
Diarrhea A disorder characterized by an increase in frequency and/or loose or watery bowel movements.Reference: https://coloncancersupport.colonclub.com/viewtopic.php?f=1&t=65882&p=510516#p510516
- Grade 1 -Diarrhea Increase of <4 stools per day over baseline; mild increase in ostomy output compared to baseline
- Grade 2 - Increase of 4 - 6 stools per day over baseline; moderate increase in ostomy output compared to baseline; limiting instrumental ADL (Activities of Daily Living)
- Grade 3 - Increase of >=7 stools per day over baseline; hospitalization indicated; severe increase in ostomy output compared to baseline; limiting self care ADL
- Grade 4 - Life-threatening consequences; urgent intervention indicated
Therefore, what I would recommend is for DH to have a serious conversation with his oncologist to discuss the issue of Grade 3 (Serious) side effects of Xeloda and how to recognize and control them. This should be done before the treatment regimen commences.
For example, if DH's regimen starts in early July, then the build-up of chemo in the body will be at a level sufficient to produce Grade 3 adverse events around the beginning or middle of September, i.e., around the 3rd or 4th Xeloda cycle. The first couple of cycles may not seem so bad, but experience has shown that by the 3rd or 4th cycle things become much more difficult to manage.
Also, after talking to the oncologist it would probably be a good idea to take a trip to the pharmacy and stock up on essentials that are likely be needed over the next few weeks. In DH's meeting with the oncologist, he could get some recommendations for the kinds of things that he will need to have close at hand.
Good luck! Take care ...
-
beach sunrise

- Posts: 1047
- Joined: Thu Mar 05, 2020 7:14 pm
Re: Need advice: Margins were not clear
Agree with Peregrine. Be fimiliar with side effects.
I have been on maintance xeloda for over two yrs and have not experienced any side effects so far. My dose is pretty high compared to some others.
To keep gut optimum I would suggest Turkey Tail, pre and probiotic, maybe whey protein.
I have been on maintance xeloda for over two yrs and have not experienced any side effects so far. My dose is pretty high compared to some others.
To keep gut optimum I would suggest Turkey Tail, pre and probiotic, maybe whey protein.
8/19 RC CEA 82.6 T3N0M0
5FU/rad 6 wk
IVC 75g 1 1/2 wks before surgery. Continue 2x a week
Surg 1/20 -margins T4bN1a IIIC G2 MSI- 1/20 LN+ LVI+ PNI-
pre cea 24 post 5.9
FOLFOX
7 rds 6-10 CEA 11.4 No more
CEA
7/20 11.1 8.8
8/20 7.8
9/20 8.8, 9, 8.6
10/20 8.1
11/20 8s
12/20 8s-9s
ADAPT++++ chrono
CEA
10/23/22 26.x
12/23/22 22.x
2023
1/5 17.1
1/20 15.9
3/30 14.9
6/12 13.3
8/1 2.1
Nodule RML SUV 1.3 5mm
Rolles 3 of 4 lung nodules cancer
KRAS
Chem-sens test failed Not enough ca cells to test
5FU/rad 6 wk
IVC 75g 1 1/2 wks before surgery. Continue 2x a week
Surg 1/20 -margins T4bN1a IIIC G2 MSI- 1/20 LN+ LVI+ PNI-
pre cea 24 post 5.9
FOLFOX
7 rds 6-10 CEA 11.4 No more
CEA
7/20 11.1 8.8
8/20 7.8
9/20 8.8, 9, 8.6
10/20 8.1
11/20 8s
12/20 8s-9s
ADAPT++++ chrono
CEA
10/23/22 26.x
12/23/22 22.x
2023
1/5 17.1
1/20 15.9
3/30 14.9
6/12 13.3
8/1 2.1
Nodule RML SUV 1.3 5mm
Rolles 3 of 4 lung nodules cancer
KRAS
Chem-sens test failed Not enough ca cells to test
Return to “Colon Talk - Colon cancer (colorectal cancer) support forum”
Who is online
Users browsing this forum: Google [Bot] and 379 guests