
It is very likely that much of what is recognized as LAR syndrome is actually related to what happens to the autonomic innervation of the neorectum during the course of the extensive mobilization that occurs during a LAR. The authors have observed in the operating room that after the complete mobilization and division of bowel required as part of a LAR (in preparation for a coloanal anastomosis), there are very strong contractions that randomly take place in the distal transverse and descending colon: they never start or progress into the mid- or proximal transverse colon. We have hypothesized that the disordered bowel function, known as LAR syndrome, is a result of motility changes seen in the left colon following extrinsic denervation that occurs with the extensive mobilization performed during these operations.
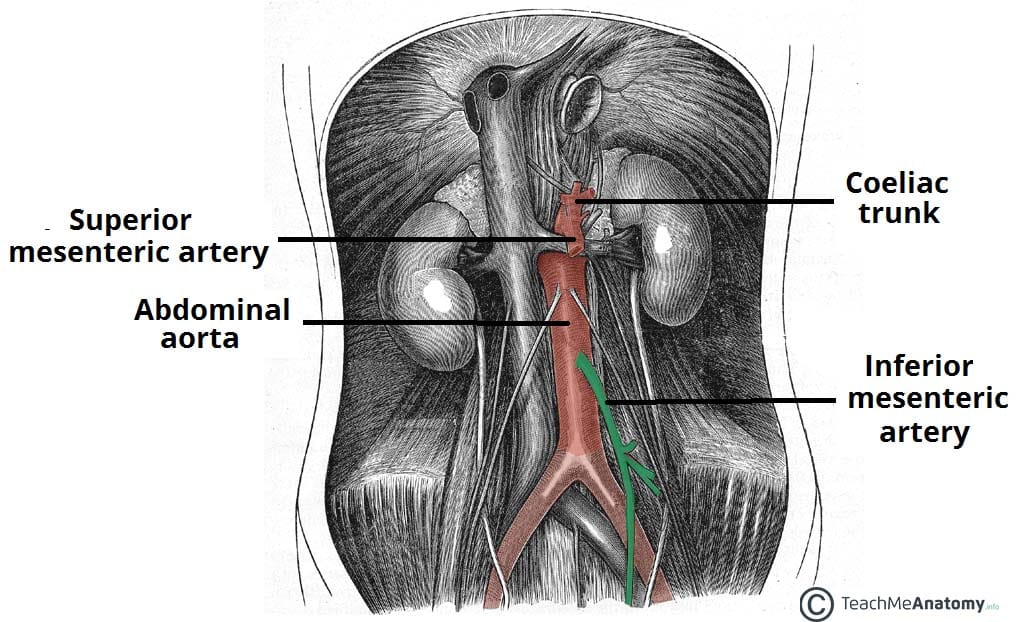
My GI doc mentioned that with the increasing popularity of laparoscopic procedures for rectal resection, very high ligation of the IMA is usually done. This is the worst possible scenario for LAR syndrome risk.
Anyone contemplating laparoscopic rectal resection should be aware of this risk and ask the surgeon about how the IMA ligation will be done. While laparoscopic surgery has a quicker recovery, it could leave one with lifelong consequences that might not happen if it's possible to choose open surgery and low ligation of the IMA. Whether that is possible or not depends on a number of factors, and can only be determined for certain during the procedure. But be informed, and discuss the risks with your doctor beforehand.


{kind=link}