Recurrent rectal cancer
Recurrent rectal cancer
Glad to have recently found the wealth of information in this forum. My husband is going through stage 2 recurrent rectal cancer (3 times), most recently finishing up 8 rounds of XELIRI, waiting for new scans and surgical consultation next week – scanxiety in full effect. CEA is on the rise and mid chemo scans showed no new growth, but also no change in tumor size. We saw the tumor sequencing panel come through but has not yet been discussed with oncologist. Looks like he has a few markers (APC, KRAS, PIC3CA). With appointments next week we want to make sure all the questions are lined up for the surgeon and oncologist. Looking for experiences and suggestions from anyone that may have a similar journey.
DW of 3 x recur rectal cancer dx 51yo
MSS w/ local recurrence - KRAS
3/2020 -3cm adenocarcinoma sigmoid pT3pN0M0
4/2020 - OLAR surgery 0/20LN (10cm from verge)
6/2021 - CT/PET - 2cm perirectal inv seminal vesicle
7/2021- 11/2021 - XELOX x6
11/2021 - 12/2021 proton therapy w/capecitabine
2/2021 - LAR Surgery - tumor only
5/2022 - CT Clear
12/2022 - PET/CT tumor sigmoid 1.8 x 1.5
1/2023 - 5/2023 XELIRI x 8
3/2023 - CT - 1.4 x 1.3
7/24 - PET 2.9 x 1.9 cm
8/18 - APR w/ total proctocolectomy and colostomy
MSS w/ local recurrence - KRAS
3/2020 -3cm adenocarcinoma sigmoid pT3pN0M0
4/2020 - OLAR surgery 0/20LN (10cm from verge)
6/2021 - CT/PET - 2cm perirectal inv seminal vesicle
7/2021- 11/2021 - XELOX x6
11/2021 - 12/2021 proton therapy w/capecitabine
2/2021 - LAR Surgery - tumor only
5/2022 - CT Clear
12/2022 - PET/CT tumor sigmoid 1.8 x 1.5
1/2023 - 5/2023 XELIRI x 8
3/2023 - CT - 1.4 x 1.3
7/24 - PET 2.9 x 1.9 cm
8/18 - APR w/ total proctocolectomy and colostomy

Re: Recurrent rectal cancer
SED wrote:... Looking for experiences and suggestions from anyone that may have a similar journey.
I'm sorry to hear about your husband's rectal recurrences. It must be very discouraging for him to have had three of these recurrences in quick succession.
I'm not sure that my journey is similar enough to your husband's for my comments to be of much value. I was Stage II-C at diagnosis with a pT4bN0M0 tumor extruding into the left seminal vesicle. I had an extensive 8-hour LAR surgery done two days after my diagnosis and it removed the primary tumor, the local lymph nodes, the left seminal vesicle and another nearby organ, with clear margins all around. After that I had 5 weeks of chemo-radiation to the pelvic area, followed by a CAPEOX regimen (capecitabine+oxaliplatin). During the subsequent 5-year follow-up period I followed a very strict self-imposed dietary and exercise program. I am now 10 years past diagnosis and I have not had any kind of recurrence, either remote or local, and have never had a CEA value higher than 1.5 ng/mL. And I have never had any genetic or genomic testing done, so I have no idea what part genetic mutations might have played in my recovery.
Your husband's journey was different from mine because he was diagnosed Stage II-A from the outset and he did not have radiation or chemo done right after his LAR surgery. This is where the main difference is, in my opinion.
If you'd like, I could give a few of my thoughts and impressions, but they would not be based on experiences like your husband has had. They would be based on second-hand information from various Stage II-A patients who have posted information on this Forum in the past.
Re: Recurrent rectal cancer
Thanks for the response and for sharing your experience.
With three recurrences in less than three years it’s been quite a whirlwind. I am open to any thoughts and impressions from others with experience. I feel like learning as much as I can about all of this is the only way I can help him.
After the first surgery and finding the second recurrence, we switched hospitals and surgeons to a larger, more well-known hospital and he is satisfied with the care they are providing. Upon finding the third recurrence, the oncologist mentioned he may be genetically pre dispositioned or the Oxaliplatin didn’t get everything.
We know little about the markers that came back on the genetic mapping (APC, KRAS, PIC3CA) . It would be nice to have some knowledge in the pocket to discuss with oncologist. He suggested the possibility of maintenance chemo if certain markers were present. Should know more about that after the upcoming appointment.
With three recurrences in less than three years it’s been quite a whirlwind. I am open to any thoughts and impressions from others with experience. I feel like learning as much as I can about all of this is the only way I can help him.
After the first surgery and finding the second recurrence, we switched hospitals and surgeons to a larger, more well-known hospital and he is satisfied with the care they are providing. Upon finding the third recurrence, the oncologist mentioned he may be genetically pre dispositioned or the Oxaliplatin didn’t get everything.
We know little about the markers that came back on the genetic mapping (APC, KRAS, PIC3CA) . It would be nice to have some knowledge in the pocket to discuss with oncologist. He suggested the possibility of maintenance chemo if certain markers were present. Should know more about that after the upcoming appointment.
DW of 3 x recur rectal cancer dx 51yo
MSS w/ local recurrence - KRAS
3/2020 -3cm adenocarcinoma sigmoid pT3pN0M0
4/2020 - OLAR surgery 0/20LN (10cm from verge)
6/2021 - CT/PET - 2cm perirectal inv seminal vesicle
7/2021- 11/2021 - XELOX x6
11/2021 - 12/2021 proton therapy w/capecitabine
2/2021 - LAR Surgery - tumor only
5/2022 - CT Clear
12/2022 - PET/CT tumor sigmoid 1.8 x 1.5
1/2023 - 5/2023 XELIRI x 8
3/2023 - CT - 1.4 x 1.3
7/24 - PET 2.9 x 1.9 cm
8/18 - APR w/ total proctocolectomy and colostomy
MSS w/ local recurrence - KRAS
3/2020 -3cm adenocarcinoma sigmoid pT3pN0M0
4/2020 - OLAR surgery 0/20LN (10cm from verge)
6/2021 - CT/PET - 2cm perirectal inv seminal vesicle
7/2021- 11/2021 - XELOX x6
11/2021 - 12/2021 proton therapy w/capecitabine
2/2021 - LAR Surgery - tumor only
5/2022 - CT Clear
12/2022 - PET/CT tumor sigmoid 1.8 x 1.5
1/2023 - 5/2023 XELIRI x 8
3/2023 - CT - 1.4 x 1.3
7/24 - PET 2.9 x 1.9 cm
8/18 - APR w/ total proctocolectomy and colostomy
Re: Recurrent rectal cancer
SED wrote:... Looks like he has a few markers (APC, KRAS, PIC3CA). With appointments next week we want to make sure all the questions are lined up for the surgeon and oncologist. Looking for experiences and suggestions from anyone that may have a similar journey ... We know little about the markers that came back on the genetic mapping (APC, KRAS, PIC3CA) . It would be nice to have some knowledge in the pocket to discuss with oncologist. He suggested the possibility of maintenance chemo if certain markers were present. Should know more about that after the upcoming appointment.
- For your meeting with the oncologist, what I would suggest is for you to print off the following list of FDA-approved drugs used to treat CRC, and to study the list so that you understand what each kind of drug is used for, and what the mechanism of actions are. Then if the oncologist proposes a particular new regimen or combination regimen then you might be better prepared to ask for clarification as to why he thinks this proposed new regimen will be any better.
https://www.empr.com/wp-content/uploads/sites/7/2020/08/FDA-Approved-Colorectal-Cancer-Treatments-0820.pdf
NOTE: This list above is almost three years old. An up-to-date list might have even more FDA-approved items on it. I'm not so sure about this. For example, there are new drugs just approved by the FDA in January 2023 that are not on the above list. They are called tucatinib (Tukysa) and trastuzumab (Herceptin) and they are for RAS wild-type, HER2-positive unresectable or metastatic colorectal cancer -- just to give an example.
For this list above of year 2020-approved drugs, it is particularly important to pay attention to Footnotes 2, 3 and 4 because they indicate which drugs are known not to work with KRAS mutant, or MSI-stable (MSS) tumors. For example, you wouldn't want the oncologist to propose trying Vectibix (panitumumab) or Erbitux (cetuximab) since it is already known that these chemo drugs don't work well when there is a KRAS mutation in the tumor --- and your husband's tumor has a KRAS mutation, so "forewarned is forearmed...". Also, checkpoint-inhibitor drugs don't work so well with patients who have MSS tumors, so you need to check whether the proposed new regimen is a checkpoint inhibitor, and, if so, whether your husband's tumor is MSI-high or MSS-low(MSS). It can make a difference.
Likewise, you need to pay attention to the drugs that have Footnote 3, because they usually only work well with tumors that are MSI-high. These drugs would be of little or no use if your husband's tumor was MSI-low or MSI-stable (MSS). By the way ... what is your husband's MSI status? This would be very important to know in scheduling any 2nd-line, 3rd-line, or 4th-line chemo options, because he wouldn't want to be put on a new regimen where his MSI-status is incompatible with the new regimen.
You should be prepared to ask for whatever clarification you need because doctors are required, by Federal law (CFR Title 21, Part 50.25), to explain all of the benefits and risks of a new treatment before the patient is asked to sign the Informed Consent form.
. - For your meeting with the surgeon, I would suggest that you ask specifically what kind of surgery is best for removing the current tumor, and ask him to show on a diagram what would be removed by the surgery and what would be the likelihood that such a surgery could be done as an 'R0 resection', i.e., a surgery that has clean margins in all directions with no cancerous tissue or cancerous droppings from the tumor left behind in the abdominal cavity during the surgery procedure.
. - With three recent local recurrences in the pelvic area, the main challenge facing the oncologist and the surgeon right now (in my opinion) is to urgently find a way to prevent the spread of cancer to the pelvic peritoneum or to the fluid in the peritoneal cavity. If spread to the peritoneum ever occurs, this is defined as "end-stage disease" with a significant shortening of life expectancy.
When cancer spreads to the peritoneum or to the peritoneal cavity it is very, very difficult to treat. This, in my opinion, is because the blood supply to these areas is very weak and no matter what kind of miracle drug you may use, it cannot reach the cancer in sufficient intensity to do any good. So, the most important thing right now is to do whatever is necessary to avoid at all cost the spread of the local recurrence into the peritoneum, a condition known as: peritoneal carcinomatosis.
. - I realize that this is a lot of material to digest on relatively short notice, but, in my opinion it is very important to deal with these issues in a timely fashion. Best of luck on your meetings with the oncologist and surgeon.
. - ADDENDUM: PIK3CA mutation"We know little about the markers that came back on the genetic mapping (APC, KRAS, PIC3CA) . It would be nice to have some knowledge in the pocket to discuss with oncologist"
For your meeting with the oncologist this week, it seems to me that a discussion of different PIK3CA mutations might be useful. This is because there were some earlier studies done in China suggesting that standard chemo doesn't work so well for certain PIK3CA mutations, and that some PIK3CA mutations are correlated with "enhanced abnormal cell proliferation and invasive ability". This might explain why the chemo done so far did not manage to prevent the three recurrences.
You can ask the oncologist what he knows about PIK3CA mutations and see what he says. He might not have had the time right now to go through all of the relevant PIK3CA articles, but at least he might know something about PIK3CA in the Western world and be able to propose a chemo regimen that would work better than the standard 1st line chemos that have been used so far. Note: There are many possible PIK3CA mutations, not just one. Similarly for KRAS: There are many possible KRAS mutations. It would be important to look closely at the genetic mapping report to see exactly what kinds of KRAS and PIK3CA mutation(s) were found, because it could make a difference in the decision-making process.
Here are references to a couple of old articles on PIK3CA and colorectal cancer.- PIK3CA mutations confer resistance to first-line chemotherapy in colorectal cancer
https://www.nature.com/articles/s41419-018-0776-6#ref-CR40
"Our study investigated the PIK3CA gene mutation and first-line chemotherapy resistance in CRC, which provide further insight in chemotherapy options. We provided evidences that PIK3CA mutation was correlated with lower histological grade, late clinical stage and poor prognosis. .. The patients with PIK3CA mutant CRC showed significant worse prognosis. Collective data suggested a potential role of mutant PIK3CA in CRC progression, which may be correlated with enhanced abnormal cell proliferation and invasive ability."
. - Prognostic role of PIK3CA mutation in colorectal cancer: cohort study and literature review
https://pubmed.ncbi.nlm.nih.gov/22357840/©2012 AACR.
"Conclusion: Coexistence of PIK3CA (the PI3K p110α subunit) exon 9 and 20 mutations, but not PIK3CA mutation in either exon 9 or 20 alone, is associated with poor prognosis of colorectal cancer patients."
- PIK3CA mutations confer resistance to first-line chemotherapy in colorectal cancer
{kind=link}
{kind=link}
Last edited by Jacques on Wed May 10, 2023 3:37 am, edited 16 times in total.
Re: Recurrent rectal cancer
Originally diagnosed with stage 4, with liver mets, he had “progression” last year. He had been on a w&w plan for about 1 1/2 yr. A suspicious cyst was discovered during a routine physical exam. Then a colonoscopy was ordered later that week. Then a CT and MRI. MRI indicated that the site of the original primary tumor, which was believed to have been destroyed with chemo and radiation, had grown. It showed potential invasion the prostrate.
There were some doubts because those MRI results could be mistaken for radiation damage. So an ultrasound was ordered with several biopsies, including a fine needle aspiration. The surface samples turned up with no cancer, but the FNA did come back positive for cancer cells. The ultrasound results showed that there was no prostrate invasion.
He was offered 3 options: chemo, a LAR, or an APR. The surgeon recommended the APR. Chemo wasn’t expected to result in a cure, The LAR would result in poor quality of life, pretty much guaranteed, and while the APR would mean adjusting to a permanent colostomy, it would be the best possible outcome. If I’m not mistaken, he was restaged with T3N0M0.
All this was about a year ago, and the APR surgery was on 5/31/2022.
Ultimately the surgery was successful and a urologist was on hand in case the prostate was involved. It was determined that the prostate did not have to be removed, but the surgery went all the way to the prostate (as far as possible, Denonvillier’s fascia). The results showed no lymph node involvement which seemed to be the biggest concern, the margins were clear on both ends, but unfortunately the circumferential margin showed cancer cells at a very small location. The urologist said heat from the cauterizing might have killed any cells that might have been past the margin, but there’s no way of knowing. Furthermore, the area where the cells would have been was unlikely to support cancer cell growth because it’s more of a layer of fat…
The oncologist recommended a 6 month course of Xeloda, and everyone else recommended no chemo. The sentiment was that he most likely would not have a recurrence. He went with the oncologists recommendation and did 6 months of chemo, ending on 1/1/2023. It was considered “insurance”.
So far he’s had a CT+MRI in Jan and then again in April. So far he’s still NED.
There were some doubts because those MRI results could be mistaken for radiation damage. So an ultrasound was ordered with several biopsies, including a fine needle aspiration. The surface samples turned up with no cancer, but the FNA did come back positive for cancer cells. The ultrasound results showed that there was no prostrate invasion.
He was offered 3 options: chemo, a LAR, or an APR. The surgeon recommended the APR. Chemo wasn’t expected to result in a cure, The LAR would result in poor quality of life, pretty much guaranteed, and while the APR would mean adjusting to a permanent colostomy, it would be the best possible outcome. If I’m not mistaken, he was restaged with T3N0M0.
All this was about a year ago, and the APR surgery was on 5/31/2022.
Ultimately the surgery was successful and a urologist was on hand in case the prostate was involved. It was determined that the prostate did not have to be removed, but the surgery went all the way to the prostate (as far as possible, Denonvillier’s fascia). The results showed no lymph node involvement which seemed to be the biggest concern, the margins were clear on both ends, but unfortunately the circumferential margin showed cancer cells at a very small location. The urologist said heat from the cauterizing might have killed any cells that might have been past the margin, but there’s no way of knowing. Furthermore, the area where the cells would have been was unlikely to support cancer cell growth because it’s more of a layer of fat…
The oncologist recommended a 6 month course of Xeloda, and everyone else recommended no chemo. The sentiment was that he most likely would not have a recurrence. He went with the oncologists recommendation and did 6 months of chemo, ending on 1/1/2023. It was considered “insurance”.
So far he’s had a CT+MRI in Jan and then again in April. So far he’s still NED.
DH 61
2019 4A t3 n2 m1a
8/23 C-scopy, 5+cm mass. CEA:4.1
9/16 MSS. MRI: 2 lvr mets: 2.7 & 7mm
9/30 Start FOLFOX 1-6
10/4 Lg lvr met ~3.7cm, pri tmr stable.
CEA: 10/13,12.5;10/27-12/8 btw 4.7 & 3.1
11/5 both lvr mets ~ 2/3 smaller.
12/17 PET: significant improv.
2020
MWA 2/5, Lap resection 2/11
CEA: 3/1-5/31 btw 2.1&2.9
3/2 start FOLFOX 7-12
7/23-29 EBRT
10/2/2020 NED/W&W
4/2022 EUS-FNA,MRI: recur.;
5/2022:CT scan no mets. APR.
7-12/2023 Xeloda
4/2023 CT/MRI NED
2019 4A t3 n2 m1a
8/23 C-scopy, 5+cm mass. CEA:4.1
9/16 MSS. MRI: 2 lvr mets: 2.7 & 7mm
9/30 Start FOLFOX 1-6
10/4 Lg lvr met ~3.7cm, pri tmr stable.
CEA: 10/13,12.5;10/27-12/8 btw 4.7 & 3.1
11/5 both lvr mets ~ 2/3 smaller.
12/17 PET: significant improv.
2020
MWA 2/5, Lap resection 2/11
CEA: 3/1-5/31 btw 2.1&2.9
3/2 start FOLFOX 7-12
7/23-29 EBRT
10/2/2020 NED/W&W
4/2022 EUS-FNA,MRI: recur.;
5/2022:CT scan no mets. APR.
7-12/2023 Xeloda
4/2023 CT/MRI NED
Re: Recurrent rectal cancer
Thanks for all of the information, it was very helpful.
Scan update - new bloodclot in the lung. Putting him on Eliquis. Nothing new in abdomen, little movment in tumor size.
CT Chest: +CRITICAL RESULT: New pulmonary embolism [CV11].
CT Abomen / Pelvis: Status post low anterior resection with colorectal anastomosis in the lower pelvis. Stable implant along the lateral aspect of the sigmoid colon measuring 1.3 x 1.0 cm
Oncologist explained that these bloodclots sometimes happen with chemo and likely traveled up from leg. He plans to attack it with high dose eliquis for a week and then down to normal dosage. DH has surgical consult tomorrow - I'm wondering how much this new clot is going to impact surgery. Tumor is considered MSI Stable. Oncologist will be doing Signatera testing on this tumor after surgery - just starting to learn about this very interesting testing. May need to resume chemo if surgery is more than 4 weeks out.
Meet with surgeon tomorrow. Plan to discuss approach, new lung clot, and prevention methods from spread to peritoneum.
Scan update - new bloodclot in the lung. Putting him on Eliquis. Nothing new in abdomen, little movment in tumor size.
CT Chest: +CRITICAL RESULT: New pulmonary embolism [CV11].
CT Abomen / Pelvis: Status post low anterior resection with colorectal anastomosis in the lower pelvis. Stable implant along the lateral aspect of the sigmoid colon measuring 1.3 x 1.0 cm
Oncologist explained that these bloodclots sometimes happen with chemo and likely traveled up from leg. He plans to attack it with high dose eliquis for a week and then down to normal dosage. DH has surgical consult tomorrow - I'm wondering how much this new clot is going to impact surgery. Tumor is considered MSI Stable. Oncologist will be doing Signatera testing on this tumor after surgery - just starting to learn about this very interesting testing. May need to resume chemo if surgery is more than 4 weeks out.
Meet with surgeon tomorrow. Plan to discuss approach, new lung clot, and prevention methods from spread to peritoneum.
DW of 3 x recur rectal cancer dx 51yo
MSS w/ local recurrence - KRAS
3/2020 -3cm adenocarcinoma sigmoid pT3pN0M0
4/2020 - OLAR surgery 0/20LN (10cm from verge)
6/2021 - CT/PET - 2cm perirectal inv seminal vesicle
7/2021- 11/2021 - XELOX x6
11/2021 - 12/2021 proton therapy w/capecitabine
2/2021 - LAR Surgery - tumor only
5/2022 - CT Clear
12/2022 - PET/CT tumor sigmoid 1.8 x 1.5
1/2023 - 5/2023 XELIRI x 8
3/2023 - CT - 1.4 x 1.3
7/24 - PET 2.9 x 1.9 cm
8/18 - APR w/ total proctocolectomy and colostomy
MSS w/ local recurrence - KRAS
3/2020 -3cm adenocarcinoma sigmoid pT3pN0M0
4/2020 - OLAR surgery 0/20LN (10cm from verge)
6/2021 - CT/PET - 2cm perirectal inv seminal vesicle
7/2021- 11/2021 - XELOX x6
11/2021 - 12/2021 proton therapy w/capecitabine
2/2021 - LAR Surgery - tumor only
5/2022 - CT Clear
12/2022 - PET/CT tumor sigmoid 1.8 x 1.5
1/2023 - 5/2023 XELIRI x 8
3/2023 - CT - 1.4 x 1.3
7/24 - PET 2.9 x 1.9 cm
8/18 - APR w/ total proctocolectomy and colostomy
Re: Recurrent rectal cancer
Update from surgeon…
First meeting with the new surgeon - DH regular surgeon is out on maternity leave. We were able to get in with the head of colorectal surgery because she consulted his case during the second surgery. The meeting went well. She was very thorough and patient and is a very highly regarded surgeon. DH felt very comfortable and so did I.
The scans were reviewed, and tumor believed to not be implanted in sidewall but has likely attached to colon. Since the previous LAR was very low (10cm) and the new tumor is a much higher, there is a significant amount of colon that will need to be removed. If there is enough and she can reattach below previous anastomosis, she will place a temporary ileostomy. If there is not enough and re-attachment is not possible, he will have permanent colostomy. The surgeon wanted to meet with the oncologist and present at tumor board again this Monday 5/15 before scheduling or making final decision on surgery. Not concered about PE. Looks like more information to come next week. If they do proceed with surgery, it looks like mid-June.
First meeting with the new surgeon - DH regular surgeon is out on maternity leave. We were able to get in with the head of colorectal surgery because she consulted his case during the second surgery. The meeting went well. She was very thorough and patient and is a very highly regarded surgeon. DH felt very comfortable and so did I.
The scans were reviewed, and tumor believed to not be implanted in sidewall but has likely attached to colon. Since the previous LAR was very low (10cm) and the new tumor is a much higher, there is a significant amount of colon that will need to be removed. If there is enough and she can reattach below previous anastomosis, she will place a temporary ileostomy. If there is not enough and re-attachment is not possible, he will have permanent colostomy. The surgeon wanted to meet with the oncologist and present at tumor board again this Monday 5/15 before scheduling or making final decision on surgery. Not concered about PE. Looks like more information to come next week. If they do proceed with surgery, it looks like mid-June.
DW of 3 x recur rectal cancer dx 51yo
MSS w/ local recurrence - KRAS
3/2020 -3cm adenocarcinoma sigmoid pT3pN0M0
4/2020 - OLAR surgery 0/20LN (10cm from verge)
6/2021 - CT/PET - 2cm perirectal inv seminal vesicle
7/2021- 11/2021 - XELOX x6
11/2021 - 12/2021 proton therapy w/capecitabine
2/2021 - LAR Surgery - tumor only
5/2022 - CT Clear
12/2022 - PET/CT tumor sigmoid 1.8 x 1.5
1/2023 - 5/2023 XELIRI x 8
3/2023 - CT - 1.4 x 1.3
7/24 - PET 2.9 x 1.9 cm
8/18 - APR w/ total proctocolectomy and colostomy
MSS w/ local recurrence - KRAS
3/2020 -3cm adenocarcinoma sigmoid pT3pN0M0
4/2020 - OLAR surgery 0/20LN (10cm from verge)
6/2021 - CT/PET - 2cm perirectal inv seminal vesicle
7/2021- 11/2021 - XELOX x6
11/2021 - 12/2021 proton therapy w/capecitabine
2/2021 - LAR Surgery - tumor only
5/2022 - CT Clear
12/2022 - PET/CT tumor sigmoid 1.8 x 1.5
1/2023 - 5/2023 XELIRI x 8
3/2023 - CT - 1.4 x 1.3
7/24 - PET 2.9 x 1.9 cm
8/18 - APR w/ total proctocolectomy and colostomy
Re: Recurrent rectal cancer
SED wrote:... Meet with surgeon tomorrow. Plan to discuss approach, new lung clot, and prevention methods from spread to peritoneum.
Thanks for the update. I imagine that DH's appointment with the surgeon has already taken place (I'm not sure what you meant by "tomorrow" because you didn't specify the date). In any event, I have other comments about surgeons and surgical techniques, but I suppose that these comments can wait until the next surgery consult. It looks like surgery is not imminent, at least not this week.
Meanwhile, I have some comments of an administrative nature.
- You need to post at least 5 to 10 posts here before they will promote you to "Registered User" status with expanded privileges. Your posts are now delayed by a number of hours because you are now only a "Newly Registered User" with just 3 posts, so your new posts still have to go through the Moderator review process and that takes time. When you finally get promoted to "Registered User" status your posts will appear on the main board as soon as you successfully Submit them. So, it is to your advantage to post messages more frequently so that you can be promoted soon and have more posting privileges here.
- There are some other things that could be added to your signature that would make it more complete. For example;
-- Baseline CEA value, if you have it.
--Location of the primary rectal tumor (i.e., cm. fom the anal verge, or low/middle/high rectum, etc.)
-- What type of LAR surgery was it - Open surgery, laparascopic surgery, or robotic surgery?
-- Did the surgery also involve a temporary ileostomy while the anastomosis was healing?
--Did the LAR pathology report mention anything about clear surgical margins?
-- What kind of CT scans were they? with contrast? without contrast?
--Does your new hospital have access to the original baseline CT scans from the first hospital?
--What kind of genetic profiling was done? Was it based only on the primary tumor biopsy? Did they ever consider doing a test of DH's inherited DNA (hereditary genetic profiling based on blood sample, etc.)
Also, some other points of information:
-What kind of surgeon did the original LAR surgery? Was he a board-certified colorectal surgeon or only a general surgeon?
-What kind of surgeon is the new surgeon and what are his qualifications and experience?
-For the Signatera test, does the oncologist have a lot of experience with this test, and will he be able to explain how the test comes up with its personalized 16 reference oncogenes? And will he be able to tell whether the DNA fragments being tracked have any relation to the mutations found in the genetic profiling report? See this post for more information:
https://coloncancersupport.colonclub.com/viewtopic.php?f=1&t=65557&p=509082#p509082
Re: Recurrent rectal cancer
You can ask the oncologist what he knows about PIK3CA mutations and see what he says. He might not have had the time right now to go through all of the relevant PIK3CA articles, but at least he might know something about PIK3CA in the Western world and be able to propose a chemo regimen that would work better than the standard 1st line chemos that have been used so far. Note: There are many possible PIK3CA mutations, not just one. Similarly for KRAS: There are many possible KRAS mutations. It would be important to look closely at the genetic mapping report to see exactly what kinds of KRAS and PIK3CA mutation(s) were found, because it could make a difference in the decision-making process.
Here are references to a couple of old articles on PIK3CA and colorectal cancer.
- PIK3CA mutations confer resistance to first-line chemotherapy in colorectal cancer
https://www.nature.com/articles/s41419-018-0776-6#ref-CR40
"Our study investigated the PIK3CA gene mutation and first-line chemotherapy resistance in CRC, which provide further insight in chemotherapy options. We provided evidences that PIK3CA mutation was correlated with lower histological grade, late clinical stage and poor prognosis. .. The patients with PIK3CA mutant CRC showed significant worse prognosis. Collective data suggested a potential role of mutant PIK3CA in CRC progression, which may be correlated with enhanced abnormal cell proliferation and invasive ability."
.- Prognostic role of PIK3CA mutation in colorectal cancer: cohort study and literature review
https://pubmed.ncbi.nlm.nih.gov/22357840/©2012 AACR.
"Conclusion: Coexistence of PIK3CA (the PI3K p110α subunit) exon 9 and 20 mutations, but not PIK3CA mutation in either exon 9 or 20 alone, is associated with poor prognosis of colorectal cancer patients."
I was able to ask some questions about DH markers from the report - had no idea what I was talking about and probably sounded like it as well but went for it anyway.
Inquired about any correlation between these APC markers and AFAP possibility – he said not likely.
APC – R213
APC – R1399
I asked about aspirin therapy related to the PIK3CA – something to investigate.
PIK3CA - E542K
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9250486/
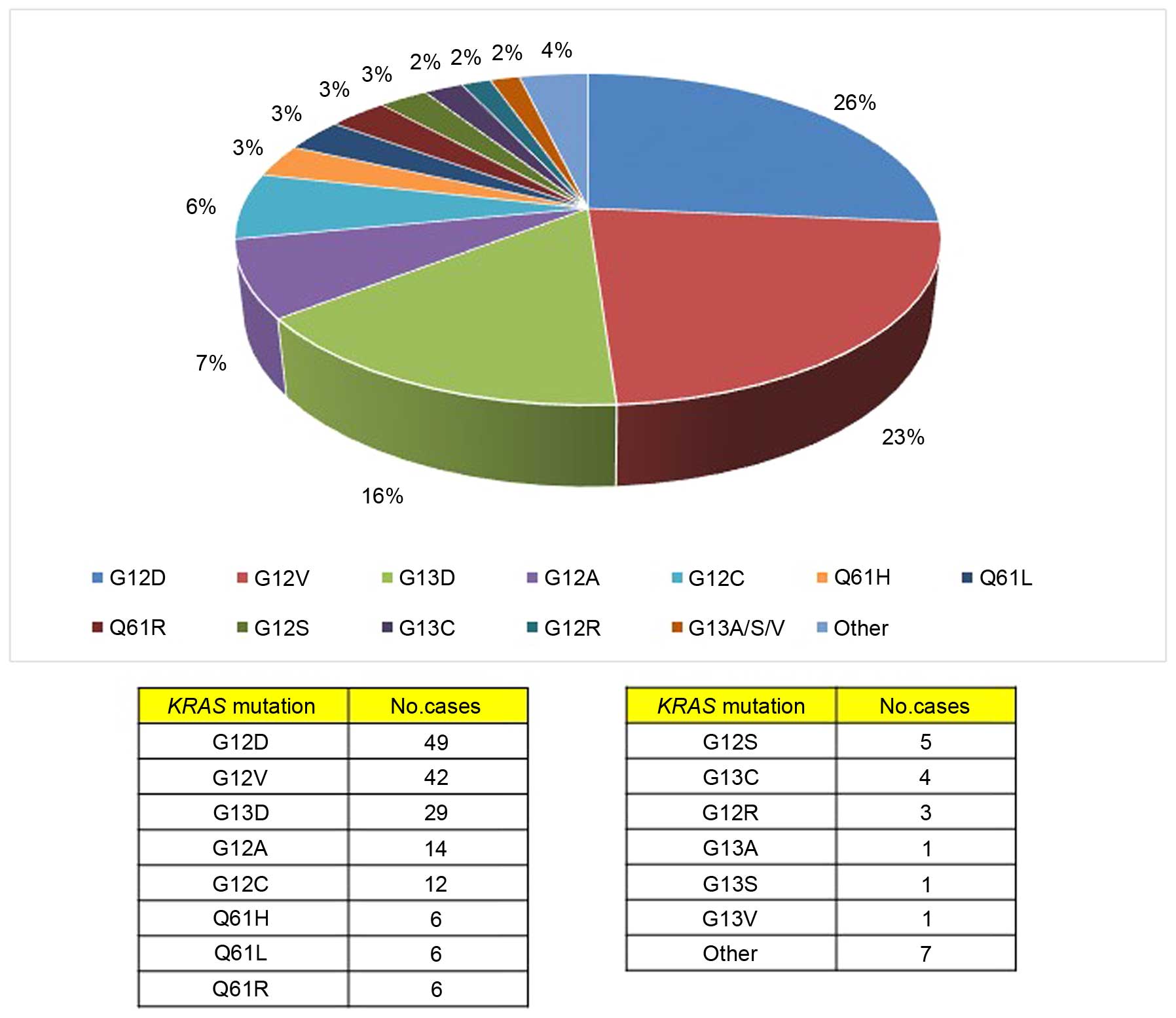
We spoke about the KRAS G12V and how there a no specific drugs for this variant unlike KRAS G12C. I inquired about IV vitamin C for this mutation. Something to investigate.
KRAS - G12V
DW of 3 x recur rectal cancer dx 51yo
MSS w/ local recurrence - KRAS
3/2020 -3cm adenocarcinoma sigmoid pT3pN0M0
4/2020 - OLAR surgery 0/20LN (10cm from verge)
6/2021 - CT/PET - 2cm perirectal inv seminal vesicle
7/2021- 11/2021 - XELOX x6
11/2021 - 12/2021 proton therapy w/capecitabine
2/2021 - LAR Surgery - tumor only
5/2022 - CT Clear
12/2022 - PET/CT tumor sigmoid 1.8 x 1.5
1/2023 - 5/2023 XELIRI x 8
3/2023 - CT - 1.4 x 1.3
7/24 - PET 2.9 x 1.9 cm
8/18 - APR w/ total proctocolectomy and colostomy
MSS w/ local recurrence - KRAS
3/2020 -3cm adenocarcinoma sigmoid pT3pN0M0
4/2020 - OLAR surgery 0/20LN (10cm from verge)
6/2021 - CT/PET - 2cm perirectal inv seminal vesicle
7/2021- 11/2021 - XELOX x6
11/2021 - 12/2021 proton therapy w/capecitabine
2/2021 - LAR Surgery - tumor only
5/2022 - CT Clear
12/2022 - PET/CT tumor sigmoid 1.8 x 1.5
1/2023 - 5/2023 XELIRI x 8
3/2023 - CT - 1.4 x 1.3
7/24 - PET 2.9 x 1.9 cm
8/18 - APR w/ total proctocolectomy and colostomy
Re: Recurrent rectal cancer
SED wrote:... Meet with surgeon tomorrow. Plan to discuss approach, new lung clot, and prevention methods from spread to peritoneum.
Thanks for the update. I imagine that DH's appointment with the surgeon has already taken place (I'm not sure what you meant by "tomorrow" because you didn't specify the date). In any event, I have other comments about surgeons and surgical techniques, but I suppose that these comments can wait until the next surgery consult. It looks like surgery is not imminent, at least not this week.
Meanwhile, I have some comments of an administrative nature.
Jacques wrote:- You need to post at least 5 to 10 posts here before they will promote you to "Registered User" status with expanded privileges. Your posts are now delayed by a number of hours because you are now only a "Newly Registered User" with just 3 posts, so your new posts still have to go through the Moderator review process and that takes time. When you finally get promoted to "Registered User" status your posts will appear on the main board as soon as you successfully Submit them. So, it is to your advantage to post messages more frequently so that you can be promoted soon and have more posting privileges here.
Good to know. I was wondering why there was a delay!
- There are some other things that could be added to your signature that would make it more complete.
For example;
Jacques wrote:-- Baseline CEA value, if you have it.
There have been 23 CEA tests and results for DH since 3/2020. I am not sure which one would be considered baseline, but I am assuming the lowest number after resection (3.6). It seems to climb during chemo – up to 8.9. The second tumor was identified only by CEA increasing to 4.5 and triggered an early scan. The third was identified by a routine follow up CT and corresponding CEA was only 3.6. So I am not sure what the actual baseline would be.
Jacques wrote:--Location of the primary rectal tumor (i.e., cm. fom the anal verge, or low/middle/high rectum, etc.)
-- What type of LAR surgery was it - Open surgery, laparascopic surgery, or robotic surgery?
-- Did the surgery also involve a temporary ileostomy while the anastomosis was healing?
--Did the LAR pathology report mention anything about clear surgical margins?
The location of the primary rectal tumor from 4/2020 was 10cm from anal verge…very low. The surgeon went into the surgery with a plan to use DaVinci robotic method. However, during the lap procedure he was unable to reach and had to open. The 2-hour planned surgery turned into 7 hours. He did not require a temporary ileostomy. The report showed clear margins.
A year later they found a new tumor in the location described below - not really near the orginaly location. This was first treated with chemo (Oxaliplatin and Capecitabine), then daily proton beam therapy (30 sessions while taking capecitabine), then finally surgery. The surgery was open LAR in the location location below. Plan was to remove significant colon and have a temp ileostomy. However, surgeon was able to resect tumor with clear margins without resecting any colon.
second recurrence: soft tissue nodule in the right perirectal space abutting the posterolateral aspect of the right seminal vesicle. currently measures 2.5 x 1.8 cm
Jacques wrote:-- What kind of CT scans were they? with contrast? without contrast?
--Does your new hospital have access to the original baseline CT scans from the first hospital?
All of the records from the old hospital were electronically sent and / or uploaded to the new hospital. Every time DH goes for a CT it is with contrast. He gets both a chest CT with contrast and a Abdominal/Pelvis CT with contrast. Since 3/2020 DH has had 13 CT w/contrast, 3 PET scans, 3 MRI
Jacques wrote:--What kind of genetic profiling was done? Was it based only on the primary tumor biopsy? Did they ever consider doing a test of DH's inherited DNA (hereditary genetic profiling based on blood sample, etc.)
DH had genetic profiling completed via blood sample and it came back clear. Met with genetic counselor and said no concern. The primary tumor biopsy was also sent for solid tumor sequencing panel and found 4 disease associated variants and 4 variants of uncertain significance. After the next surgery the tumor will be sent for cfDNA testing.
Jacques wrote:Also, some other points of information:
-What kind of surgeon did the original LAR surgery? Was he a board-certified colorectal surgeon or only a general surgeon?
-What kind of surgeon is the new surgeon and what are his qualifications and experience?
-For the Signatera test, does the oncologist have a lot of experience with this test, and will he be able to explain how the test comes up with its personalized 16 reference oncogenes? And will he be able to tell whether the DNA fragments being tracked have any relation to the mutations found in the genetic profiling report? See this post for more information:
https://coloncancersupport.colonclub.com/viewtopic.php?f=1&t=65557&p=509082#p509082
The original LAR surgery was done at our local hospital by a surgeon who was referred to us by the facility that did the original screening colonoscopy. He was a surgeon in an office of colorectal surgeons. When I look, I do not see him listed on the ASCRS website but I do see another surgeon in that office listed. Is there another site to check for this certification?
The new surgeon is highly qualified, the chief of colorectal surgery, and on the executive board of the ASCRS.
Highly confident with oncologist and cfDNA testing and interpreting results.
DW of 3 x recur rectal cancer dx 51yo
MSS w/ local recurrence - KRAS
3/2020 -3cm adenocarcinoma sigmoid pT3pN0M0
4/2020 - OLAR surgery 0/20LN (10cm from verge)
6/2021 - CT/PET - 2cm perirectal inv seminal vesicle
7/2021- 11/2021 - XELOX x6
11/2021 - 12/2021 proton therapy w/capecitabine
2/2021 - LAR Surgery - tumor only
5/2022 - CT Clear
12/2022 - PET/CT tumor sigmoid 1.8 x 1.5
1/2023 - 5/2023 XELIRI x 8
3/2023 - CT - 1.4 x 1.3
7/24 - PET 2.9 x 1.9 cm
8/18 - APR w/ total proctocolectomy and colostomy
MSS w/ local recurrence - KRAS
3/2020 -3cm adenocarcinoma sigmoid pT3pN0M0
4/2020 - OLAR surgery 0/20LN (10cm from verge)
6/2021 - CT/PET - 2cm perirectal inv seminal vesicle
7/2021- 11/2021 - XELOX x6
11/2021 - 12/2021 proton therapy w/capecitabine
2/2021 - LAR Surgery - tumor only
5/2022 - CT Clear
12/2022 - PET/CT tumor sigmoid 1.8 x 1.5
1/2023 - 5/2023 XELIRI x 8
3/2023 - CT - 1.4 x 1.3
7/24 - PET 2.9 x 1.9 cm
8/18 - APR w/ total proctocolectomy and colostomy
Certification of surgeons
SED wrote:...The original LAR surgery was done at our local hospital by a surgeon who was referred to us by the facility that did the original screening colonoscopy. He was a surgeon in an office of colorectal surgeons. When I look, I do not see him listed on the ASCRS website but I do see another surgeon in that office listed. Is there another site to check for this certification?
- You could try the https://www.certificationmatters.org website.
* Put in only the last name of the doctor.
* Select one of the specialties below.
- Colon & Rectal Surgery
- Surgery
- Complex General Surgical Oncology
. - You could try the http://www.absurgery.org/ website.
* Put in only the last name of the doctor.
This website is for General Surgery certification.
Re: Recurrent rectal cancer
SED wrote:...With three recurrences in less than three years it’s been quite a whirlwind. I am open to any thoughts and impressions from others with experience. I feel like learning as much as I can about all of this is the only way I can help him...
Overview
This post provides a reading list addressing some of the reasons why a pT3 rectal tumor could possibly produce several local recurrences. These are not the only possible ways that a rectal tumor can trigger recurrences, but they are the main ones that can be documented through post-surgery pathology reports and various scan reports (CT and MRI scans).
If you take time to read through some of these articles and posts you can learn new vocabulary and get a better understanding of what might have happened to produce so many recurrences in such a short period of time. This may provide background for discussion with the doctors in your upcoming meetings with them.
As an introduction to this area I would suggest that you first read the post linked directly below to get a general idea of the situation for pT3 rectal tumors, and then later look at the 5 main topics listed below when you have some time.
===============================
- Lympho-Vascular Invasion (LVI)
- Prognostic value of lymphovascular invasion in stage II colorectal cancer patients with an inadequate examination of lymph nodes
https://wjso.biomedcentral.com/articles/10.1186/s12957-021-02224-3 - Perineural Invasion (PNI)
- The role of perineural invasion in predicting survival in patients with primary operable colorectal cancer: A systematic review
https://pubmed.ncbi.nlm.nih.gov/28325252/ - Extramural Vascular Invasion (EMVI)
- Extramural venous invasion in rectal cancer: overview of imaging, histopathology, and clinical implications
https://pubmed.ncbi.nlm.nih.gov/29967984/ - Tumor Deposits (TD)
- Tumor Deposits in Colorectal Cancer: Improving the Value of Modern Staging-A Systematic Review and Meta-Analysis
https://pubmed.ncbi.nlm.nih.gov/28029327/...Tumor deposits, alongside the ancillary finding of extramural venous invasion (EMVI), are increasingly recognized as being the most important predictors of distant metastatic disease, overall survival and disease-free survival for patients with rectal cancer ... - Tumor Budding (TB)
- Tumor budding in colorectal carcinoma: Time to take notice
https://mp.uscap.org/article/S0893-3952(22)02967-2/fulltext...Unfortunately, a substantial number of tumors behave poorly despite being categorized as low risk [e.g.Stage II-A] based on their TNM stage.2 Thus, the search for additional prognostic factors in the assessment of colorectal carcinoma has been a major research focus. Of the histopathological factors studied to date, the most promising include extramural venous invasion (EMVI), the nature of the advancing front (pushing vs infiltrative), an inflammatory infiltrate, microsatellite instability (MSI), and tumor budding (TB) —the presence of small discrete clusters of tumor cells at the invasive edge (Figure 1). There is now overwhelming evidence that tumor budding is an independent prognostic factor in colorectal carcinoma, particularly in node-negative (N0) disease..
P.S. I just noticed that now, with 6 posted messages, you have just been promoted finally to status of "Registered User". Congratulations! From now on you will have access to all of the main features if this message board.
Re: Recurrent rectal cancer
Not too much of an update, but the 5/15 tumor board meeing for DH was pushed to this past Monday 5/22. The outcome of that meeting was not a surgery date, but a request for another colonoscopy next week. We guess the surgeon wants to take another look before committing to his surgery. They said DH would have to wait on biopsy results from colonoscopy before determining the final plan.
DW of 3 x recur rectal cancer dx 51yo
MSS w/ local recurrence - KRAS
3/2020 -3cm adenocarcinoma sigmoid pT3pN0M0
4/2020 - OLAR surgery 0/20LN (10cm from verge)
6/2021 - CT/PET - 2cm perirectal inv seminal vesicle
7/2021- 11/2021 - XELOX x6
11/2021 - 12/2021 proton therapy w/capecitabine
2/2021 - LAR Surgery - tumor only
5/2022 - CT Clear
12/2022 - PET/CT tumor sigmoid 1.8 x 1.5
1/2023 - 5/2023 XELIRI x 8
3/2023 - CT - 1.4 x 1.3
7/24 - PET 2.9 x 1.9 cm
8/18 - APR w/ total proctocolectomy and colostomy
MSS w/ local recurrence - KRAS
3/2020 -3cm adenocarcinoma sigmoid pT3pN0M0
4/2020 - OLAR surgery 0/20LN (10cm from verge)
6/2021 - CT/PET - 2cm perirectal inv seminal vesicle
7/2021- 11/2021 - XELOX x6
11/2021 - 12/2021 proton therapy w/capecitabine
2/2021 - LAR Surgery - tumor only
5/2022 - CT Clear
12/2022 - PET/CT tumor sigmoid 1.8 x 1.5
1/2023 - 5/2023 XELIRI x 8
3/2023 - CT - 1.4 x 1.3
7/24 - PET 2.9 x 1.9 cm
8/18 - APR w/ total proctocolectomy and colostomy
Re: Recurrent rectal cancer
Update:
A colonoscopy was performed in early June. The purpose was for the surgeon to get a better look and try and biopsy. The surgeon was able to see the mass and noted that "mass adjacent to the wall of the descending colon about 25 cm proximal to his anastomosis." In late June, it was determined that surgeons were not able to get suitable tissue for the biopsy. Next step - PET scan before surgery.
The PET scan was completed and did not see anything new. However, the original tumor has increased in size since May - (2.9 x 1.9 cm, previously 1.8 x 1.5 cm). The oncologist reviewed the scan and suggested to move forward asap with the surgery due to growth.
During the first meeting with the surgeon in May, she expressed it would be a more difficult surgery than the prior two. The original anastomosis is very low (10 cm from verge) and the new tumor is 25cm higher than original anastomosis. This requires removing a significant amount of bowel. It is also located in a difficult location. She was not certain they would be possible to make a connection. Hopefully the recent colonoscopy and PET with give the team a better look and help finalize the plan.
Upcoming meeting with surgeon this week 8/2 to finalize plan and get scheduled - this will be DH third LAR in 4 years.
Daughter is getting married mid-September and the oncologist suggests surgery should happen before that time because of the growth since stopping chemo. He also suggests that additional growth could impede a muscle that would complicate the surgery. Going back on chemo short term was also not an option. The wedding is a 5-hour car ride – not sure if that is going to be possible for DH post-surgery. Thoughts on this?
A colonoscopy was performed in early June. The purpose was for the surgeon to get a better look and try and biopsy. The surgeon was able to see the mass and noted that "mass adjacent to the wall of the descending colon about 25 cm proximal to his anastomosis." In late June, it was determined that surgeons were not able to get suitable tissue for the biopsy. Next step - PET scan before surgery.
The PET scan was completed and did not see anything new. However, the original tumor has increased in size since May - (2.9 x 1.9 cm, previously 1.8 x 1.5 cm). The oncologist reviewed the scan and suggested to move forward asap with the surgery due to growth.
During the first meeting with the surgeon in May, she expressed it would be a more difficult surgery than the prior two. The original anastomosis is very low (10 cm from verge) and the new tumor is 25cm higher than original anastomosis. This requires removing a significant amount of bowel. It is also located in a difficult location. She was not certain they would be possible to make a connection. Hopefully the recent colonoscopy and PET with give the team a better look and help finalize the plan.
Upcoming meeting with surgeon this week 8/2 to finalize plan and get scheduled - this will be DH third LAR in 4 years.
Daughter is getting married mid-September and the oncologist suggests surgery should happen before that time because of the growth since stopping chemo. He also suggests that additional growth could impede a muscle that would complicate the surgery. Going back on chemo short term was also not an option. The wedding is a 5-hour car ride – not sure if that is going to be possible for DH post-surgery. Thoughts on this?
DW of 3 x recur rectal cancer dx 51yo
MSS w/ local recurrence - KRAS
3/2020 -3cm adenocarcinoma sigmoid pT3pN0M0
4/2020 - OLAR surgery 0/20LN (10cm from verge)
6/2021 - CT/PET - 2cm perirectal inv seminal vesicle
7/2021- 11/2021 - XELOX x6
11/2021 - 12/2021 proton therapy w/capecitabine
2/2021 - LAR Surgery - tumor only
5/2022 - CT Clear
12/2022 - PET/CT tumor sigmoid 1.8 x 1.5
1/2023 - 5/2023 XELIRI x 8
3/2023 - CT - 1.4 x 1.3
7/24 - PET 2.9 x 1.9 cm
8/18 - APR w/ total proctocolectomy and colostomy
MSS w/ local recurrence - KRAS
3/2020 -3cm adenocarcinoma sigmoid pT3pN0M0
4/2020 - OLAR surgery 0/20LN (10cm from verge)
6/2021 - CT/PET - 2cm perirectal inv seminal vesicle
7/2021- 11/2021 - XELOX x6
11/2021 - 12/2021 proton therapy w/capecitabine
2/2021 - LAR Surgery - tumor only
5/2022 - CT Clear
12/2022 - PET/CT tumor sigmoid 1.8 x 1.5
1/2023 - 5/2023 XELIRI x 8
3/2023 - CT - 1.4 x 1.3
7/24 - PET 2.9 x 1.9 cm
8/18 - APR w/ total proctocolectomy and colostomy
Return to “Colon Talk - Colon cancer (colorectal cancer) support forum”
Who is online
Users browsing this forum: No registered users and 265 guests