rp1954 wrote:I need a few more questions and data. I am going start with some observations and comparisons.
I would be happy to to answer all your questions and provide data if I have it. Your help and advice is highly appreciated.
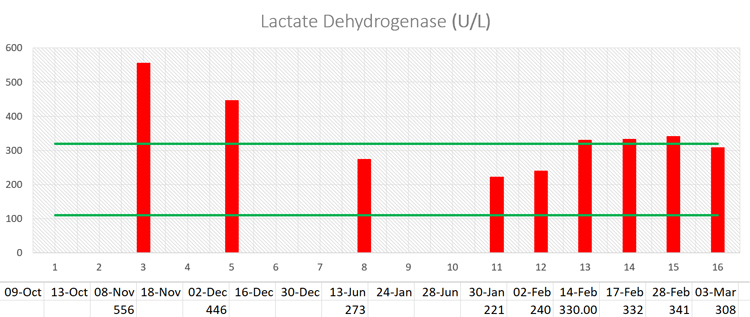
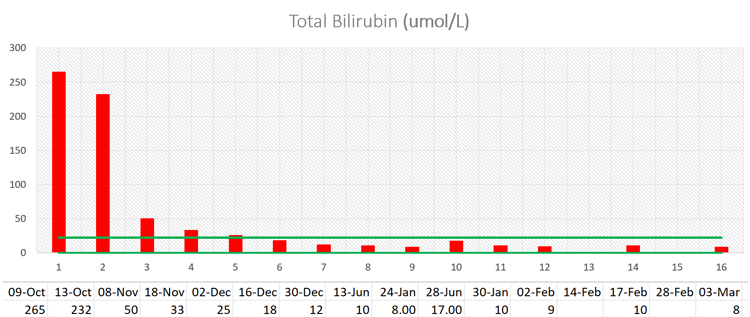
rp1954 wrote:Likewise her LDH is hovering in the 200s up to 300 now and could be a combined effect of chemo and IVC. The 2nd half of February data, LDH around UL might be flu, set it aside for the moment.
Ideally LDH is below 170 for mCRC patients with previously elevated LDH, a potential curative sign.
mCRC with elevated LDH and HIF-1a, due to anaerobic sugar metabolism elevates LDH into the 200s and beyond, like with your wife's early data
I have a couple more LDH results from the end of 2022: 0ct.19 - 1897, Oct.24 - 1002, Nov.04 - 556, Dec.02 - 446
rp1954 wrote:One natural question is what is your wife's optimum IV vitamin C, where C is known to accumulate in KRAS cancer cells and disrupt KRAS and HIF-1a metabolism.
That is a good question. Riordan IVC Protocol Research (
https://riordanclinic.org/research-stud ... -protocol/) says "therapeutic goal of reaching a peak-plasma concentration of ~20 mM (350- 400 mg/dL) is most efficacious".
After 50g vit C (1.1g/kg), her level is 16-18. After 75g (1.35g/kg) - 22-24. Freshly compounded C gives 10-20% higher respond.
Her usual IVC protocol is 3 times per week - 2x 75g and 1x 50g. Also Riordan says "No increased toxicity for post-IVC plasma vitamin C levels up to 780 mg/dL has been observed" - it is about 40-42 mM, so we have enough room to increase.
rp1954 wrote:With my wife's small cancer tissue chunks in suspension, 5FU+C+K2 beat 5FU+oxi and/or iri, to the great dismay of the lab.
What is the name of this test and where it can be done? This seems to be a very important test for treatment strategy.
rp1954 wrote:90g/m2 is roughly 40-50% higher than the 1.5 grams/kg UL dose usually used by oncology NDs.
Her Body Surface Area is 1.6 - 1.67 based on different formulas, so 90g/m2 is 144 - 150g. Pretty high dose.
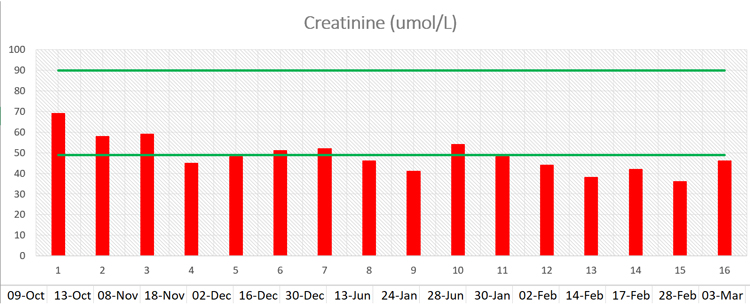
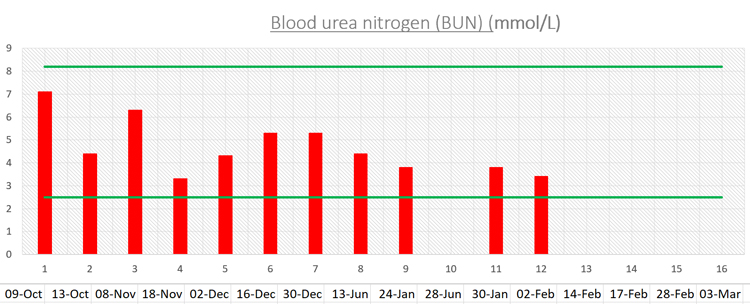
rp1954 wrote:So what does your wife's kidney data series look like?
Unfortunately we didn't GFR test. I only have Creatinine and BUN for kidneys
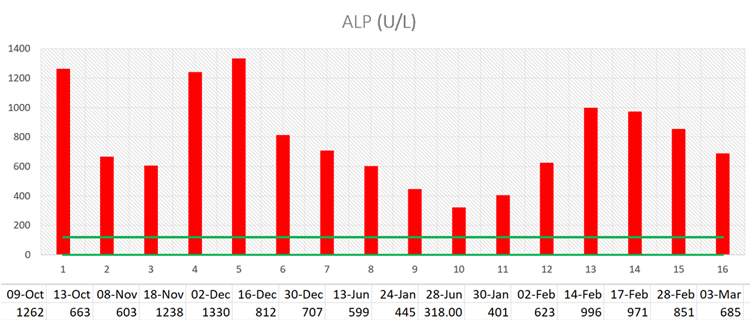
rp1954 wrote:AST (aka SGOT) is so common in liver panels (AST+ALT+ALP) of std and cheapo blood chemistry packages, I'm amazed if it's not in your drs data. A caregiver reference item if they don't start it.
I missed it. I ask third party doctor for requisition for extended tests I'd like to order, and no one check them except me. For our onc standard blood work is enough. I get much more info here from that forum than from him.
rp1954 wrote:I'd get at least one AFP for reference. It a cheap old marker.
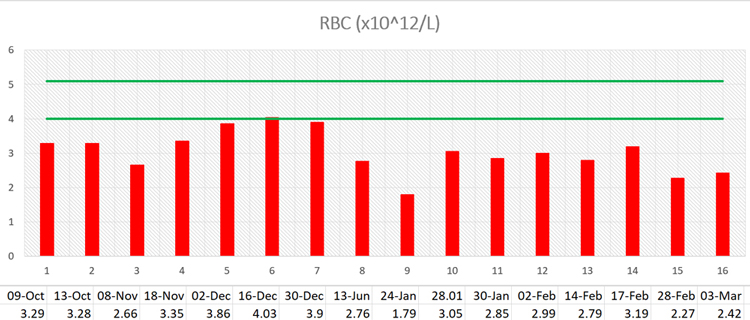
Reticulocytes, "Retics" are immature RBC. They were added when the RBC got low.
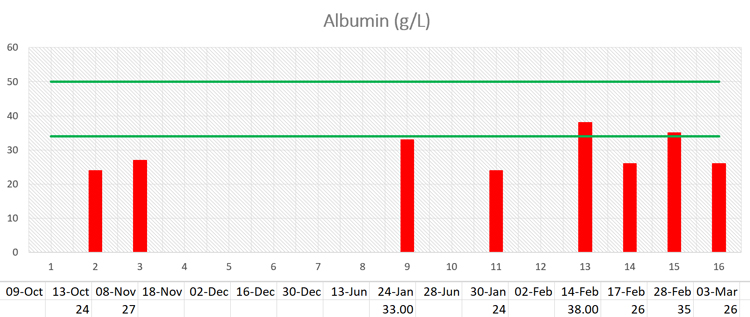
Albumin is the most important protein lab, but I'd ask the onc for better cover with Total Protein A/G.
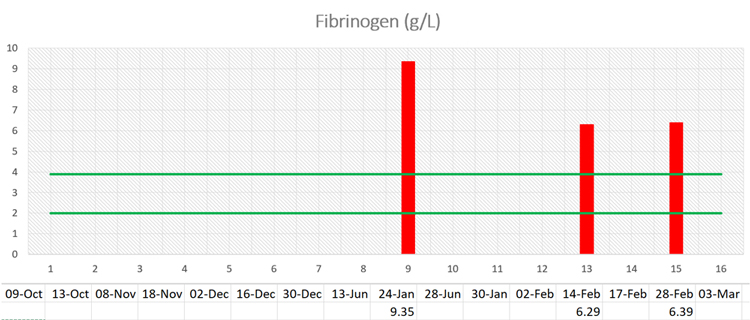
Also I'd get d-dimer and cortisol.
Thanks, will ask to add.
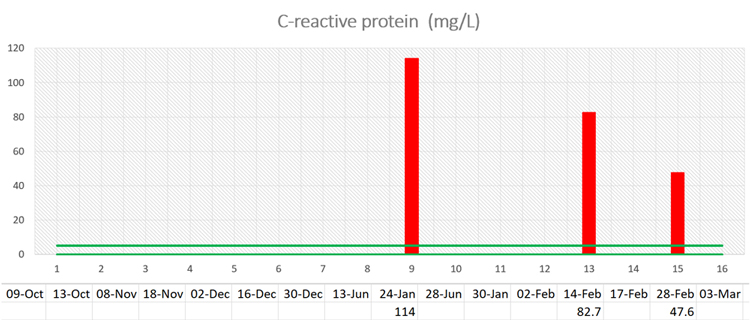
I did D-dimer a couple last tests - it's too high (Feb.14 - 1931, Feb.28 - 1500). UL is 500.
rp1954 wrote:Finally, what are the Folfox dose changes and change dates?
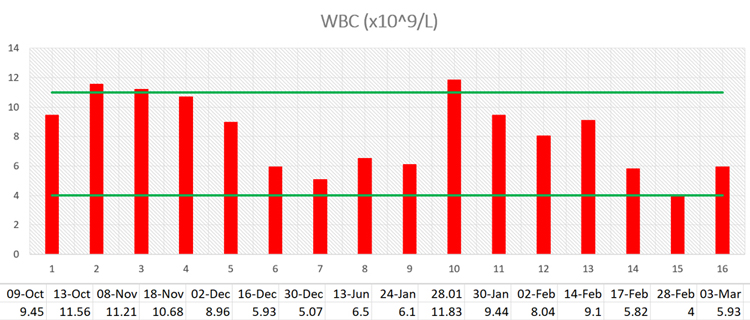
Any WBC or RBC colony stimulation factors yet?
In late January it looks dose reduction and/or some Neupogen/Neulasta.
No, nothing extra.
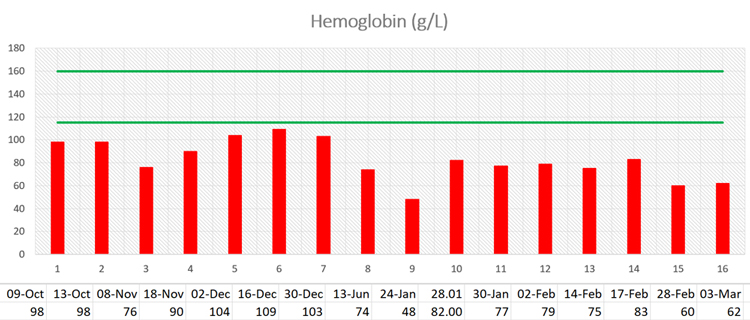
ND started low dose IM testosterone (25 mg/weekly) last week try to boost Hgb. That is off-label of course.