Newly diagnosed stage I may be? Rectal cancer
-
Beenumehta
- Posts: 10
- Joined: Mon Jun 20, 2022 9:14 pm
Newly diagnosed stage I may be? Rectal cancer
Just got diagnosed wiith low rectal cancer 3-4 cm from anal verge. Looking for options divided between local anal excision and total mesorectal excision. Confused and scared? Anyone out there who has done local anal excision and had good outcome?
Female age 51 at Dx CRa ~4 cm from anal verge
Blood in stool March 2022
Colonoscopy May 11,2022
Rectum polypectomy 2 cm polyp
Pathology report Mucinous adenocarcinoma, moderately differentiated, involving colonic mucosa with positive margin
MRI and CT scan clear
Aug 4,22 LAR surgery
December 8, 2023 reversal
Previous thyroidectomy at age 50 for papillary carcinoma surgery Jan 2021 partial April 2021 complete .
RAI August 2021
Blood in stool March 2022
Colonoscopy May 11,2022
Rectum polypectomy 2 cm polyp
Pathology report Mucinous adenocarcinoma, moderately differentiated, involving colonic mucosa with positive margin
MRI and CT scan clear
Aug 4,22 LAR surgery
December 8, 2023 reversal
Previous thyroidectomy at age 50 for papillary carcinoma surgery Jan 2021 partial April 2021 complete .
RAI August 2021

Re: Newly diagnosed stage I may be? Rectal cancer
Beenumehta wrote:Just got diagnosed wiith low rectal cancer 3-4 cm from anal verge. Looking for options divided between local anal excision and total mesorectal excision. Confused and scared? Anyone out there who has done local anal excision and had good outcome?
Hello Beenumehta, and welcome to the Club... and thanks for preparing your signature in advance. That will help a lot in understanding your situation.
It looks like you have already had cancer experience with your thyroid problem, and now you have to start dealing with rectal cancer !! Sometimes things just happen like this, but I don't know why. Just a string of bad luck that we have to confront and overcome.
To answer your question, yes there are people here who have had trans-anal excisions done. I don't know about your location, but in the U.S. there are specialized clinics and hospitals that have equipment and expertise for doing what is called Trans Anal Endoscopic Microsurgery (TEM). I think there is one member here who just had another transanal excision procedure done, but in his case he calls the procedure TAE (Trans Anal Excision?). Since he has had this very same procedure done before, he might be able to comment on how the earlier TAEs turned out.
https://coloncancersupport.colonclub.com/viewtopic.php?f=1&t=66243#p512854
Also, there is a member here who had a local rectal excision done 15 years ago and has not had any problems since that time:
https://coloncancersupport.colonclub.com/viewtopic.php?f=1&t=53498&p=490399&hilit=excision#p490399
You can review all the different options for removing small rectal cancers in the following post:
https://coloncancersupport.colonclub.com/viewtopic.php?f=1&t=66167&p=512290#p512290
Keep in mind that the trans-anal approach might only be possible if the tumor is low in the rectum, because if it is too high up the endoscopic equipment might not reach that high. But there are other ways to remove small tumors if the doctors have the right kind of equipment and if the doctors are highly competent and experienced in this kind of procedure.
-
roadrunner
- Posts: 466
- Joined: Sun Jan 12, 2020 8:46 pm
Re: Newly diagnosed stage I may be? Rectal cancer
This is a difficult question. I had a TAE for what was then viewed as Stage III disease (an existing lung nodule later turned out to be a met). But I also had TNT and chemoradiation, and achieved a near-complete clinical response. Additionally, my approach has definitely not been SOC, and I chose it with that knowledge (I have a great, pioneering surgeon who has kept me well informed of the risks throughout, and this was my call). So far, so good. Just had another TAE for a villous adenoma which appeared benign, but we’ll see.
Your situation is a little unclear, but appears very different from mine. For that reason, I’m hesitant to offer any advice other than to say that it’s something I would research and get second opinions on. There are options, but each comes with its own risks/rewards. Good luck!
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4397248/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4194025/
Your situation is a little unclear, but appears very different from mine. For that reason, I’m hesitant to offer any advice other than to say that it’s something I would research and get second opinions on. There are options, but each comes with its own risks/rewards. Good luck!
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4397248/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4194025/
7/19: RC: Staged IIIA, T2N1M0
approx 4.25 cm, low/mid rectum, mod. well diff.; lung micronodule
8/19-10/19 4 rds.FOLFOX neoadjuvant, 3 w/Oxiplatin (reduced 70-75%)
neoadjuvant chemorad 11/19
4 rounds FOLFOX July-August 2020
ncCR 10/20; biopsies neg
TAE 11/20, tumor cells removed
Chest CT 3/30/21 growth in 2 nodules (3 and 5mm)
VATS 12/8/21 sub-pleural met 7mm.
SBRT nodule 1/22
6/20/22 TAE rectal polyp benign)
NED from 3/22 - 3/23
4 cycles FOLFIRI
LUL VATS lobectomy for radio resistant met 7/7/23
approx 4.25 cm, low/mid rectum, mod. well diff.; lung micronodule
8/19-10/19 4 rds.FOLFOX neoadjuvant, 3 w/Oxiplatin (reduced 70-75%)
neoadjuvant chemorad 11/19
4 rounds FOLFOX July-August 2020
ncCR 10/20; biopsies neg
TAE 11/20, tumor cells removed
Chest CT 3/30/21 growth in 2 nodules (3 and 5mm)
VATS 12/8/21 sub-pleural met 7mm.
SBRT nodule 1/22
6/20/22 TAE rectal polyp benign)
NED from 3/22 - 3/23
4 cycles FOLFIRI
LUL VATS lobectomy for radio resistant met 7/7/23
Re: Newly diagnosed stage I may be? Rectal cancer
Beenumehta wrote:Just got diagnosed wiith low rectal cancer 3-4 cm from anal verge. Looking for options divided between local anal excision and total mesorectal excision. Confused and scared? Anyone out there who has done local anal excision and had good outcome?
Beenumehta -
Your signature says:
- Female age 51 at diagnosis
Blood in stool March 2022
Colonoscopy May 11,2022
Rectum polypectomy 2 cm polyp
Pathology report Mucinous adenocarcinoma, moderately differentiated, involving colonic mucosa with positive margin
MRI and ct scan clear
Looking for options?
Previous thyroidectomy at age 50 for papillary carcinoma surgery Jan 21 partial April 21 complete .
RAI August 21
In the diagram below you can see that there are 4 layers in the rectum wall:
1. Mucosa (innermost layer)
2. Sub-mucosa
3. Muscularis
4. Serosa (outermost layer)
According to your signature, your 2 cm polyp involved the innermost layer, the "mucosa". You can see from the diagram below that this layer does not have a lot of large blood vessels or neural connections. It's the deeper layers that have the major lymphovascular and neural connections. Thus, you could assume that this polyp, although malignant, was probably not involved with shedding many cancer cells to other parts of the body. So it is probably "only" a Stage I tumor, and probably amenable to some kind of endoscopic excision or endoscopic dissection to remove what was left in the "positive margin" after the polypectomy.
But there is always the possibility that a few malignant cells left the polyp and traveled elsewhere before the bulk of the polyp was removed, or even that some cancerous cells were "dropped" during the procedure while the polyp was being removed. So, this is where the dilemma is: Do you decide to do a simple excision now to scoop out just that area of the mucosa where the polyp was found, or do you do a more extensive removal involving other, deeper, layers of the rectum wall, just in case the cancerous polyp had grown deeper than what the colonoscopy biopsy suggested. In the most extreme case you could do a full-blown TME-based LAR which would likely remove everything that might have been infiltrated, including nearby lymph nodes.
One possible problem with just doing a local excision is that the outer rectum wall and the adjacent lymph nodes would not be removed, thus the pathology report of the surgery would not have any information at all on these outer areas since they weren't part of the specimen sent to the pathologist.
So, this is where you need to get the best advice possible, and do whatever additional scans or tests necessary to determine just how invasive the polyp was. I don't know what additional procedures or technology might need to be involved, but it could be something like an MRI with contrast, or a trans-anal ultrasound, or something else to get additional data on the likely depth of the polyp root. Also, it could be important to know exactly what type of polyp was removed, e.g., a flat (sessile) polyp, or a pedunculated polyp with a central root, or a donut-shaped polyp, etc. It might make a difference in how deeply into the wall the polyp was growing. Also important is to know the type of growth pattern in the polyp, e.g., "tubular" vs. "tubulovillous" vs. "villous", etc.
So, it seems to me that quite a lot of additional research and testing will need to be done before you can safely proceed with something like a simple local excision. You may need to get second and third opinions on how best to proceed, especially since the recent polypectomy was essentially a failure since it had positive margins and no doubt left left some difficult scar tissue behind as well as some cancer cells, which will be more troublesome to deal with now than just a simple local excision for a polyp.
Also, it would be good if you could have a look at the two articles that roadrunner mentioned earlier (first two listed below), plus a third summary article.
Local excision for early rectal cancer: transanal endoscopic microsurgery and beyond
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4397248/
When is local excision appropriate for "early" rectal cancer?
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4194025/
Endoscopic management of complex colorectal polyps: Current insights and future trends
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8811151/
I would also suggest reading the article below, in addition, since it addresses the current (2020) standards for managing malignant colorectal polyps:
Endoscopic Recognition and Management Strategies for Malignant Colorectal Polyps: Recommendations of the US Multi-Society Task Force on Colorectal Cancer
https://www.gastrojournal.org/article/S0016-5085(20)35122-2/fulltext
.

-
Beenumehta
- Posts: 10
- Joined: Mon Jun 20, 2022 9:14 pm
Re: Newly diagnosed stage I may be? Rectal cancer
My 2 cm polyp was sessile and removed with a hot snare. So far I had pathology of polyp read by 4 different places. Tumor present at the cauterized edge (inked margin) . Tumor involves the entire submucosa a(for at least 6 mm) and is present in cauterized margin. Immunostains for mismatch repair protein are reviewed and intact. No lymphovascular invasion was identified.
MRI of pelvis and abdomen and CT Scan was also done with and without contrast. I was given first option to do full resection surgery and remove whole rectum and part of sigmoid colon since it is very low. Temporary ileostomy may be later reversal. Second option was wait and watch with close monitoring. So far I am on wait and watch and it is nerve wracking and any simple pain is causing panic attacks. Feel like I am playing Russian roulette with my life. I am schedule for repeat flex sig and MRI in end of August.
Other surgeon wants to do just Local anal excision and remove 1 cm around the polyp and 1/2 cm deep.
MRI of pelvis and abdomen and CT Scan was also done with and without contrast. I was given first option to do full resection surgery and remove whole rectum and part of sigmoid colon since it is very low. Temporary ileostomy may be later reversal. Second option was wait and watch with close monitoring. So far I am on wait and watch and it is nerve wracking and any simple pain is causing panic attacks. Feel like I am playing Russian roulette with my life. I am schedule for repeat flex sig and MRI in end of August.
Other surgeon wants to do just Local anal excision and remove 1 cm around the polyp and 1/2 cm deep.
Female age 51 at Dx CRa ~4 cm from anal verge
Blood in stool March 2022
Colonoscopy May 11,2022
Rectum polypectomy 2 cm polyp
Pathology report Mucinous adenocarcinoma, moderately differentiated, involving colonic mucosa with positive margin
MRI and CT scan clear
Aug 4,22 LAR surgery
December 8, 2023 reversal
Previous thyroidectomy at age 50 for papillary carcinoma surgery Jan 2021 partial April 2021 complete .
RAI August 2021
Blood in stool March 2022
Colonoscopy May 11,2022
Rectum polypectomy 2 cm polyp
Pathology report Mucinous adenocarcinoma, moderately differentiated, involving colonic mucosa with positive margin
MRI and CT scan clear
Aug 4,22 LAR surgery
December 8, 2023 reversal
Previous thyroidectomy at age 50 for papillary carcinoma surgery Jan 2021 partial April 2021 complete .
RAI August 2021
Re: Newly diagnosed stage I may be? Rectal cancer
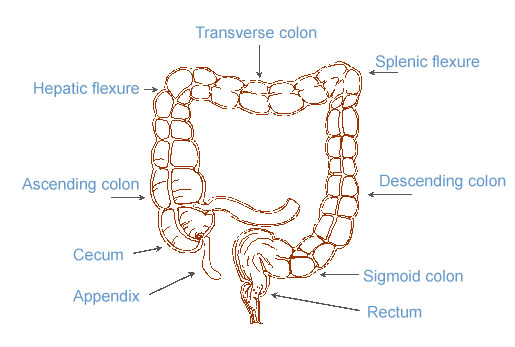
Beenumehta wrote:Just got diagnosed with low rectal cancer 3-4 cm from anal verge. Looking for options divided between local anal excision and total mesorectal excision. Confused and scared? Anyone out there who has done local anal excision and had good outcome?
The average colon is about 1.5 m long. Lengths of the various parts are (very) approximately:
* Ascending colon: 20 - 25 cm
* Transverse colon: 45 cm
* Descending colon: 10 - 15 cm
* Sigmoid colon: 35 - 40 cm
* Rectum: 12 cm
* Anal canal: 4 - 5 cm
* Anal verge: 0
Reference: https://training.seer.cancer.gov/colorectal/anatomy/
-----------------------------------------------------------------------------------------------------------------
{kind=link}
Beenumehta -
Actually, I'm a bit confused now, too. I guess I don't understand where your 2 cm polyp was actually located. If it was only 3-4 cm from the anal verge, then it could have been entirely within the anal canal, below the anal sphincter (at least according to the SEER training manual diagram). If so, this would classify the polyp as an anal polyp, not as a rectal polyp, and the cancer would be called "anal cancer". However, if the polyp was located entirely above the anal sphincter, then it would be called a rectal polyp and the cancer would be called "rectal cancer".
Would you be able to clarify this? I think it might be important because the histology of the rectum (mainly epithelial cells) is different from the histology of the anal canal (mainly squamous cells), and the two types of cancer are different, and the protocol guidelines for treating these two types of cancer are different. Also, if you know how far the edge of the polyp was from the sphincter, that would help clarify things, too.
I'm sorry I didn't notice this earlier, but there must be some great variation in lengths of anal canals across the population of patients. I just saw another source that claims the female anal canal averages about 2 cm to 3 cm in length. I don't know who to believe now.
You said that the "Other surgeon wants to do just Local anal excision ..." and that confused me, too, since I'm not sure if he is referring to doing an excision in the anal canal or not. Is this the same doctor who did the original polypectomy? Also, do you have a Medical Oncologist assigned to your case, and do you have a Radiation Oncologist assigned to your case? What kinds of doctors are on your medical team?
Thank you.
-
roadrunner
- Posts: 466
- Joined: Sun Jan 12, 2020 8:46 pm
Re: Newly diagnosed stage I may be? Rectal cancer
I think Peregrine has asked a valid question, but I suspect the confusion simply results from confusion about the term “anal verge,” or something similar, so I’m going to assume this is a rectal issue.
There are a couple of things of note in the information you provided. First, I think the mucinous component, fragmentary removal, and positive margins should be discussed with your surgeon and or medical oncologist in relation to your current approach, which you described as “watch and wait.” I would want to be sure that those don’t present significant risks in that context, or at least risks you don’t want to run (it is ultimately up to the patient, but I believe in being optimally informed). I would ask these questions to your team (I go as far to ask about odds of recurrence, for example.) Second, you expressed extreme stress around your current strategy, even to the extent of “panic attacks.” As a patient who has been on a W&W protocol for some time, I well understand this. Scans, labs, and procedures can create real anxiety. The approach is not for everyone. (The term “scanxiety” is familiar to many of us.) In my case, I get a bit nervous, but mostly the day of the scan, etc. Otherwise, I try to exercise as much as possible, play music, have fun. Only you know how difficult your stress is, or if there might be ways to get on top of it, but I would not want to have too much stress for too long over this strategic choice. Extreme stress of some sorts is associated with metastasis in animal studies. That’s not to scare you more, but just to say that you’re really in pretty good shape now (no metastasis), and it would likely be best to settle on a plan you’re comfortable with. If you can’t get reassurance on the W&W in light of the three factors above (and any other relevant concerns, including your risk tolerance), then you seem to have two other potentially reasonable strategies, one quite conservative (TME), and one in the middle (local excision). Hope this helps, and good luck!
P.S. I understand that your situation is scary, but I meant what I said above—it sounds like it is quite promising and manageable. I wish you strength in addressing it both medically and psychologically. : )
There are a couple of things of note in the information you provided. First, I think the mucinous component, fragmentary removal, and positive margins should be discussed with your surgeon and or medical oncologist in relation to your current approach, which you described as “watch and wait.” I would want to be sure that those don’t present significant risks in that context, or at least risks you don’t want to run (it is ultimately up to the patient, but I believe in being optimally informed). I would ask these questions to your team (I go as far to ask about odds of recurrence, for example.) Second, you expressed extreme stress around your current strategy, even to the extent of “panic attacks.” As a patient who has been on a W&W protocol for some time, I well understand this. Scans, labs, and procedures can create real anxiety. The approach is not for everyone. (The term “scanxiety” is familiar to many of us.) In my case, I get a bit nervous, but mostly the day of the scan, etc. Otherwise, I try to exercise as much as possible, play music, have fun. Only you know how difficult your stress is, or if there might be ways to get on top of it, but I would not want to have too much stress for too long over this strategic choice. Extreme stress of some sorts is associated with metastasis in animal studies. That’s not to scare you more, but just to say that you’re really in pretty good shape now (no metastasis), and it would likely be best to settle on a plan you’re comfortable with. If you can’t get reassurance on the W&W in light of the three factors above (and any other relevant concerns, including your risk tolerance), then you seem to have two other potentially reasonable strategies, one quite conservative (TME), and one in the middle (local excision). Hope this helps, and good luck!
P.S. I understand that your situation is scary, but I meant what I said above—it sounds like it is quite promising and manageable. I wish you strength in addressing it both medically and psychologically. : )
7/19: RC: Staged IIIA, T2N1M0
approx 4.25 cm, low/mid rectum, mod. well diff.; lung micronodule
8/19-10/19 4 rds.FOLFOX neoadjuvant, 3 w/Oxiplatin (reduced 70-75%)
neoadjuvant chemorad 11/19
4 rounds FOLFOX July-August 2020
ncCR 10/20; biopsies neg
TAE 11/20, tumor cells removed
Chest CT 3/30/21 growth in 2 nodules (3 and 5mm)
VATS 12/8/21 sub-pleural met 7mm.
SBRT nodule 1/22
6/20/22 TAE rectal polyp benign)
NED from 3/22 - 3/23
4 cycles FOLFIRI
LUL VATS lobectomy for radio resistant met 7/7/23
approx 4.25 cm, low/mid rectum, mod. well diff.; lung micronodule
8/19-10/19 4 rds.FOLFOX neoadjuvant, 3 w/Oxiplatin (reduced 70-75%)
neoadjuvant chemorad 11/19
4 rounds FOLFOX July-August 2020
ncCR 10/20; biopsies neg
TAE 11/20, tumor cells removed
Chest CT 3/30/21 growth in 2 nodules (3 and 5mm)
VATS 12/8/21 sub-pleural met 7mm.
SBRT nodule 1/22
6/20/22 TAE rectal polyp benign)
NED from 3/22 - 3/23
4 cycles FOLFIRI
LUL VATS lobectomy for radio resistant met 7/7/23
-
roadrunner
- Posts: 466
- Joined: Sun Jan 12, 2020 8:46 pm
Re: Newly diagnosed stage I may be? Rectal cancer
Sorry—should have added: Depth of submucosal invasion (“at least 6mm”) and location (low in the rectum) also appear to be risk factors for metastasis.
7/19: RC: Staged IIIA, T2N1M0
approx 4.25 cm, low/mid rectum, mod. well diff.; lung micronodule
8/19-10/19 4 rds.FOLFOX neoadjuvant, 3 w/Oxiplatin (reduced 70-75%)
neoadjuvant chemorad 11/19
4 rounds FOLFOX July-August 2020
ncCR 10/20; biopsies neg
TAE 11/20, tumor cells removed
Chest CT 3/30/21 growth in 2 nodules (3 and 5mm)
VATS 12/8/21 sub-pleural met 7mm.
SBRT nodule 1/22
6/20/22 TAE rectal polyp benign)
NED from 3/22 - 3/23
4 cycles FOLFIRI
LUL VATS lobectomy for radio resistant met 7/7/23
approx 4.25 cm, low/mid rectum, mod. well diff.; lung micronodule
8/19-10/19 4 rds.FOLFOX neoadjuvant, 3 w/Oxiplatin (reduced 70-75%)
neoadjuvant chemorad 11/19
4 rounds FOLFOX July-August 2020
ncCR 10/20; biopsies neg
TAE 11/20, tumor cells removed
Chest CT 3/30/21 growth in 2 nodules (3 and 5mm)
VATS 12/8/21 sub-pleural met 7mm.
SBRT nodule 1/22
6/20/22 TAE rectal polyp benign)
NED from 3/22 - 3/23
4 cycles FOLFIRI
LUL VATS lobectomy for radio resistant met 7/7/23
Trans-anal excision vs. trans-abdominal resection ?
roadrunner wrote:... but just to say that you’re really in pretty good shape now (no metastasis), and it would likely be best to settle on a plan you’re comfortable with...
P.S. I understand that your situation is scary, but I meant what I said above—it sounds like it is quite promising and manageable. I wish you strength in addressing it both medically and psychologically. : )
Beenumehta -
I totally agree with roadrunner who, as always, has very good technical and emotional advice. For now, you are in a good situation and you should try not to worry too much -- if you can manage to focus your thoughts on other things. But there are still some red flags in your pathology report that need to be addressed eventually before you decide on what to do next.
I think it might be a good idea for you to look at the NCCN standard of care for rectal polyps, since that would give you a reference point from which you can collect your thoughts. Apparently there is a 2017 version of the Guidelines that is still accessible on-line, so you can get a good idea of the issues at hand and the sequence of decision-making actions required at this point in your cancer journey. Just click on the Rectal Cancer Guidelines (2017) link below.
Rectal Cancer Guidelines (2017)
https://www2.tri-kobe.org/nccn/guideline/colorectal/english/rectal.pdf
In your case, the relevant pages are the ones related to rectal polyps, which you can find in the following sections of the 153-page document.:
- Principles of Pathologic Review (REC-A, 6 pages)
REC-A is found on page 21 of the 153 page document.
Be sure to read all of the relevant pages of this section because any high-risk factors from pathology are what are important for you right now.
. - Sessile Polyp (adenoma) with Invasive Cancer (REC-1)
REC-1 is found on page 10 of the 153 page document
In this section there is a branch labeled "Fragmented specimen, or margin cannot be assessed or unfavorable histological features which then leads to two different possible choices, "Trans-anal Excision, if appropriate" and "Trans-abdominal Resection". These two choices are then described in REC-2 and then in REC-B
. - REC-2 - Initial work-up for Clinical Stages T1-2,N0 :
REC-2 is found on page 11 of the 153 page document.
- This page shows the first branch of the decision tree for the various clinical stages.
. - REC-B - Principles of Surgery (Page 1 only)
REC-B, Page 1 is found on page 27 of the 153 page document.
- This page discusses minimal criteria for Trans-anal excision (e.g.,TAE, TAM, TAMIS, TASER, etc.) vs. Trans-abdominal resection (e.g., ULAR, LAR, TME, etc.)
●●● NOTE: This is the page that discusses minimal criteria for the choices that you are pondering over at the moment, i.e., Trans-anal excision vs. Trans-abdominal resection. Be sure to read all of the comments on that page, and maybe some of the footnotes, too.
.
Then, much later, after your have decided on and have had one of these two types of surgery, there is the possibility for post-surgery (i.e., adjuvant) treatment:
. - REC-3 (Treatment after Trans-anal Excision - cT1,2-N0 ) and REC-4 (Treatment after Trans-abdominal Resection - cT1,2-N0 ). These are the sections most relevant for your consideration much later in time, maybe next year.
- Adjuvant Treatment: "Treatment after Trans-Anal Excision - cT1,2-N0 tumor " (REC-3)
- Adjuvant Treatment: "Treatment after Trans-Abdominal Resection - cT1,2-N0 tumor" (REC-4)
======
Also, whenever you get the time, it would be good to have a look at this post and its embedded links:
https://coloncancersupport.colonclub.com/viewtopic.php?f=1&t=60733&p=480975#p480975
Polypectomy pathology report
Beenumehta wrote:My 2 cm polyp was sessile and removed with a hot snare. So far I had pathology of polyp read by 4 different places...
Beenumehta -
If you have a printed copy of your pathology report, could you compare what's in your report to what a polypectomy pathology report is supposed to contain according to current reporting standards? (See three-page summary of reporting standards in the document below.)
Does your report contain all of the required details?
A Guide to Polypectomy and Local Resections of the Colorectum Histopathology Reporting
https://www.rcpa.edu.au/Library/Practising-Pathology/Structured-Pathology-Reporting-of-Cancer/Cancer-Protocols/Gastrointestinal/Guide-Polypectomy-local-resections-CR
Also, if you have a printed copy of your colonoscopy report, could you evaluate the report in terms of the set of quality indicators that define a well-administered colonoscopy? (See the articles below.)
Colonoscopy: Quality Indicators
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4418496/
https://www1.nyc.gov/assets/doh/downloa ... cators.pdf
-
Beenumehta
- Posts: 10
- Joined: Mon Jun 20, 2022 9:14 pm
Re: Newly diagnosed stage I may be? Rectal cancer
Just got another opinion and new place read slides again. Pathology report Shows same mucinous features with some signet cells. Going for full mesorectal resection at MSK soon. I think this will give me and my family peace of mind. Hoping for best outcome and hopefully no complications. Fingers crossed. Wish me luck.
Thanks for all the information and help me in deciding.
Thanks for all the information and help me in deciding.
Female age 51 at Dx CRa ~4 cm from anal verge
Blood in stool March 2022
Colonoscopy May 11,2022
Rectum polypectomy 2 cm polyp
Pathology report Mucinous adenocarcinoma, moderately differentiated, involving colonic mucosa with positive margin
MRI and CT scan clear
Aug 4,22 LAR surgery
December 8, 2023 reversal
Previous thyroidectomy at age 50 for papillary carcinoma surgery Jan 2021 partial April 2021 complete .
RAI August 2021
Blood in stool March 2022
Colonoscopy May 11,2022
Rectum polypectomy 2 cm polyp
Pathology report Mucinous adenocarcinoma, moderately differentiated, involving colonic mucosa with positive margin
MRI and CT scan clear
Aug 4,22 LAR surgery
December 8, 2023 reversal
Previous thyroidectomy at age 50 for papillary carcinoma surgery Jan 2021 partial April 2021 complete .
RAI August 2021
-
Beenumehta
- Posts: 10
- Joined: Mon Jun 20, 2022 9:14 pm
Re: Newly diagnosed stage I may be? Rectal cancer
Surgery scheduled for August 4. Ultra low LAR surgery. Surgeon is saying they will not be able to use staple but will be hand sewing anastomoses. Any one has any insight on this? Is it better or not?
Female age 51 at Dx CRa ~4 cm from anal verge
Blood in stool March 2022
Colonoscopy May 11,2022
Rectum polypectomy 2 cm polyp
Pathology report Mucinous adenocarcinoma, moderately differentiated, involving colonic mucosa with positive margin
MRI and CT scan clear
Aug 4,22 LAR surgery
December 8, 2023 reversal
Previous thyroidectomy at age 50 for papillary carcinoma surgery Jan 2021 partial April 2021 complete .
RAI August 2021
Blood in stool March 2022
Colonoscopy May 11,2022
Rectum polypectomy 2 cm polyp
Pathology report Mucinous adenocarcinoma, moderately differentiated, involving colonic mucosa with positive margin
MRI and CT scan clear
Aug 4,22 LAR surgery
December 8, 2023 reversal
Previous thyroidectomy at age 50 for papillary carcinoma surgery Jan 2021 partial April 2021 complete .
RAI August 2021
Return to “Colon Talk - Colon cancer (colorectal cancer) support forum”
Who is online
Users browsing this forum: Google [Bot] and 365 guests