
I'm wondering whether or not it might be a good idea to have a special, structured checklist that newly diagnosed Stage IV patients could use just after diagnosis to make sure that everything is in order from a medical standpoint. This would be a checklist to insure that certain important things are not overlooked and do not "fall between the cracks". What do you think?
Are there any Stage IV patients out there who know about the existence of any such checklists? If so, please post information on how to access these resources.
Thank you.
Checklists for newly diagnosed Stage IV patients?
{kind=link}
-
ginabeewell

- Posts: 565
- Joined: Wed Oct 24, 2018 10:30 am
Re: Checklists for newly diagnosed Stage IV patients?
My only additional thought here is that it might make sense to have a set of checklists, so that it’s clear what needs to happen in the first weeks vs months. It can be overwhelming to get so much advice right at the beginning!
49 YO mom of twins (11) lucky stepmom of 16/19 year olds
9/17/18 DX stage 4 CRC w inoperable liver mets CEA 931
Currently NED!
Join me on a lookback of my journey via my Strive for Five on Substack here:
https://ginajacobson.substack.com
All treatment details here:
https://www.weareallmadeofstars.net/col ... nt-journey
My favorite posts here:
https://weareallmadeofstars.net/favorite-posts
9/17/18 DX stage 4 CRC w inoperable liver mets CEA 931
Currently NED!
Join me on a lookback of my journey via my Strive for Five on Substack here:
https://ginajacobson.substack.com
All treatment details here:
https://www.weareallmadeofstars.net/col ... nt-journey
My favorite posts here:
https://weareallmadeofstars.net/favorite-posts
-
Rock_Robster
- Posts: 1029
- Joined: Thu Oct 25, 2018 5:27 am
- Location: Brisbane, Australia
Re: Checklists for newly diagnosed Stage IV patients?
If a more advanced diagnosis (eg late stage III or stage IV):
Full staging including PET-CT.
Biomarker/genomics testing, including MSS/MSI and targetable mutations.
Baseline bloods including CEA and CA19-9.
Comprehensive treatment plan developed by multidisciplinary team (not just first step). Should include direct surgical consult prior to initiating treatment.
Second opinion on treatment plan (at an NCI-designated centre if in the US).
If indicated for pain / side effects - palliative care consult.
Advanced Care Planning / living will / medical power of attorney (or whatever it is where you are).
Allied health consult - psychology/social work, dental, physio/prehab, chemo or wound care/continence nurse, etc.
Financial plan - including insurance coverage and access to necessary financial support, disability, etc.
Full staging including PET-CT.
Biomarker/genomics testing, including MSS/MSI and targetable mutations.
Baseline bloods including CEA and CA19-9.
Comprehensive treatment plan developed by multidisciplinary team (not just first step). Should include direct surgical consult prior to initiating treatment.
Second opinion on treatment plan (at an NCI-designated centre if in the US).
If indicated for pain / side effects - palliative care consult.
Advanced Care Planning / living will / medical power of attorney (or whatever it is where you are).
Allied health consult - psychology/social work, dental, physio/prehab, chemo or wound care/continence nurse, etc.
Financial plan - including insurance coverage and access to necessary financial support, disability, etc.
41M Australia
2018 Dx RC
G2 EMVI LVI, 4 liver mets
pT3N1aM1a Stage IVa MSS NRAS G13R
CEA 14>2>32>16>19>30>140>70
11/18 FOLFOX
3/19 Liver resection
5/19 Pelvic IMRT
7/19 ULAR
8/19 Liver met
8/19 FOLFOX, FOLFOXIRI, FOLFIRI
12/19 Liver resection
NED 2 years
11/21 Liver met, PALN, lung nodules
3/22 PVE, lymphadenectomy, liver SBRT
10/22 PALN SBRT
11/22 Liver mets, peri nodule. Xeloda+Bev
4/23 XELIRI+Bev
9/23 ATRIUM trial
12/23 Modified FOLFIRI+Bev
3/24 VAXINIA (CF33 + hNIS) trial
2018 Dx RC
G2 EMVI LVI, 4 liver mets
pT3N1aM1a Stage IVa MSS NRAS G13R
CEA 14>2>32>16>19>30>140>70
11/18 FOLFOX
3/19 Liver resection
5/19 Pelvic IMRT
7/19 ULAR
8/19 Liver met
8/19 FOLFOX, FOLFOXIRI, FOLFIRI
12/19 Liver resection
NED 2 years
11/21 Liver met, PALN, lung nodules
3/22 PVE, lymphadenectomy, liver SBRT
10/22 PALN SBRT
11/22 Liver mets, peri nodule. Xeloda+Bev
4/23 XELIRI+Bev
9/23 ATRIUM trial
12/23 Modified FOLFIRI+Bev
3/24 VAXINIA (CF33 + hNIS) trial
Re: Checklists for newly diagnosed Stage IV patients?
Thanks to everyone for the comments, all of which are useful. As prayingforccr suggests, at this point in time we are probably at the early stages of "brainstorming" where we are collecting different ideas for analysis and classification into a small number of categories that will eventually lead to a bullet list of points that can finally lead to one or more checklists.
There are some issues or concerns with all of this, however. As Gina has already suggested, there is the problem of TMI (Too Much Information) where many newly diagnosed patients are already stressed to the limit and up to their ears with Google-search information to the point that they cannot deal with a long, comprehensive list of concerns that urgently need to be dealt with. So, this amounts to the dilemma of choosing between a long, comprehensive checklist and a much shorter one that newly diagnosed patients will actually be able to handle.
Perhaps we could first develop a comprehensive list and then decide how to prioritize it or fragment it into a smaller number of high-priority points that could be more easily addressed.
I'm not sure exactly how to deal with this. My own preference is to develop a more-or-less comprehensive master checklist and then extract subsets of this master checklist to be used for special purposes.
The main "special purpose" that I have in mind is to have a focused checklist that will help guarantee that all of the data elements, consultations and verifications necessary for developing a truly personalized Stage IV treatment plan are completed before any sort of treatment intervention is ever launched. This is to insure that the necessary thinking is done up front in order to make sure that the patient is not just routinely scheduled for a one-size-fits-all palliative standard-of-care (SOC) regimen that may turn out not to be the best possible regimen to guarantee a favorable treatment outcome in their case.
And as Rob has suggested, the initial treatment planning must be thorough and multidisciplinary in nature and must lay out, in advance, all of the sequential elements of the plan, specifying the details of what kinds of interventions (chemo, radiation, surgery) are planned and in what order, with provisions for a Plan "B" or Plan "C" in case the preferred Plan "A" fails to achieve the desired results. This multi-level plan must be based on as much relevant diagnostic data that can possibly be collected and verified in the first few weeks so as to insure that the treatment is based on complete, detailed staging information.
Right now I am in the process of translating into English and adapting a 12-point cancer checklist (published earlier this year in Europe) for my own use here as a kind of boilerplate draft to start with. Actually, the European checklist has quite a bit of overlap with the list that Rob has already given, but it needs to be adapted to the American colorectal cancer context if it is ever going to be useful in the U.S.
.
There are some issues or concerns with all of this, however. As Gina has already suggested, there is the problem of TMI (Too Much Information) where many newly diagnosed patients are already stressed to the limit and up to their ears with Google-search information to the point that they cannot deal with a long, comprehensive list of concerns that urgently need to be dealt with. So, this amounts to the dilemma of choosing between a long, comprehensive checklist and a much shorter one that newly diagnosed patients will actually be able to handle.
Perhaps we could first develop a comprehensive list and then decide how to prioritize it or fragment it into a smaller number of high-priority points that could be more easily addressed.
I'm not sure exactly how to deal with this. My own preference is to develop a more-or-less comprehensive master checklist and then extract subsets of this master checklist to be used for special purposes.
The main "special purpose" that I have in mind is to have a focused checklist that will help guarantee that all of the data elements, consultations and verifications necessary for developing a truly personalized Stage IV treatment plan are completed before any sort of treatment intervention is ever launched. This is to insure that the necessary thinking is done up front in order to make sure that the patient is not just routinely scheduled for a one-size-fits-all palliative standard-of-care (SOC) regimen that may turn out not to be the best possible regimen to guarantee a favorable treatment outcome in their case.
And as Rob has suggested, the initial treatment planning must be thorough and multidisciplinary in nature and must lay out, in advance, all of the sequential elements of the plan, specifying the details of what kinds of interventions (chemo, radiation, surgery) are planned and in what order, with provisions for a Plan "B" or Plan "C" in case the preferred Plan "A" fails to achieve the desired results. This multi-level plan must be based on as much relevant diagnostic data that can possibly be collected and verified in the first few weeks so as to insure that the treatment is based on complete, detailed staging information.
Right now I am in the process of translating into English and adapting a 12-point cancer checklist (published earlier this year in Europe) for my own use here as a kind of boilerplate draft to start with. Actually, the European checklist has quite a bit of overlap with the list that Rob has already given, but it needs to be adapted to the American colorectal cancer context if it is ever going to be useful in the U.S.
.
Re: Checklists for newly diagnosed Stage IV patients?
Hello Everyone -
Just an update to say that I am still interested in coming up with a structured checklist designed especially for newly-diagnosed Stage IV patients, but I haven't done anything on it recently. However, now that there have been a number of suggestions here on this thread, as well as on other threads, I think I can start preparing a new, enlarged draft for review.
As I mentioned earlier in the post below, I will probably work on this in two stages: First, make a single, long check-list that identifies the main check-list items. Then in the second stage, prioritize the items in that master list so that the list can then be divided into a sequence of smaller checklists that can be more easily managed by a newly-diagnosed patient.
I have already posted my edited translation of the 12-point European version of a checklist for newcomers, however that checklist is a general one, not designed specifically for stage IV patients. Now I think what I want to do is to take that 12-point checklist as a starting point to create a master checklist, focusing specifically on Stage IV-related issues -- and which would probably have about twice as many items, but with the items all prioritized
How does that sound?
Just an update to say that I am still interested in coming up with a structured checklist designed especially for newly-diagnosed Stage IV patients, but I haven't done anything on it recently. However, now that there have been a number of suggestions here on this thread, as well as on other threads, I think I can start preparing a new, enlarged draft for review.
As I mentioned earlier in the post below, I will probably work on this in two stages: First, make a single, long check-list that identifies the main check-list items. Then in the second stage, prioritize the items in that master list so that the list can then be divided into a sequence of smaller checklists that can be more easily managed by a newly-diagnosed patient.
I have already posted my edited translation of the 12-point European version of a checklist for newcomers, however that checklist is a general one, not designed specifically for stage IV patients. Now I think what I want to do is to take that 12-point checklist as a starting point to create a master checklist, focusing specifically on Stage IV-related issues -- and which would probably have about twice as many items, but with the items all prioritized
How does that sound?
Re: Checklists for newly diagnosed Stage IV patients?
The main "special purpose" that I have in mind is to have a focused checklist that will help guarantee that all of the data elements, consultations and verifications necessary for developing a truly personalized Stage IV treatment plan are completed before any sort of treatment intervention is ever launched. This is to insure that the necessary thinking is done up front in order to make sure that the patient is not just routinely scheduled for a one-size-fits-all palliative standard-of-care (SOC) regimen that may turn out not to be the best possible regimen to guarantee a favorable treatment outcome in their case.
One of the big problems is metastatic staging itself. Damn near got my wife killed.
Simply, many nominal stage IIIs and even IIs get nailed by misunderstandings on metastases including what staging means/misses, incomplete information, miscommunications and errors, that are relevant to actual metastatic status from an omniscient clinical view, or at least, the probability of being different stages in actuality. Probably the RCs stage situations get misunderstood most often because of neoadjuvant radiation downstaging, and the differences between clinical and pathological stage determinations.
To myself, I call this "all Mx'd up".
Note "Mx" itself was removed or deprecated in AJCC ca 2010 but the practical problem of "what am I really," persists for the patient. In my eyes the actual staging problem was actually aggravated by demanding an M0 or M1, rather than stating a probability or substantial uncertainty. The patient needs can be quite different than "today's" medical protocol needs or task, insurance, or drs "to do".
From the start, I realized that a lot of imperfections, problems and missed opportunities were occurring in real time on diagnostic information. I launched my inquiries into additional blood data with growing dissatisfaction as I asked more doctors with blank looks. Then I took two years to flesh the relevant panels with the medical literature that yield stage probabilities (for rough estimates) for a particular panel or combination in various conditions.
This staging concern came to a head with the sudden and tragic death of Starbuck. I realized then that patients needed more independent, much better information than "std" because the drs not only couldn't see (or wouldn't tell us), much less stop the bullet in mid flight. In Starbuck30's case, they missed a rolling cannonball. (In the US Revolutionary War, some poor americans would "dance" at the edge of cannon fire to collect the slowing and rolling cannon balls' metal for ammo) I was traumatized by "Starbuck's surprise," being so badly blindsided. For months, I worried and searched the medical literature for panels to see such potential problems sooner and more completely.
My advice, people need to get the more comprehensive blood data first thing.
Ideally, at moment of diagnosis by the gastroenterologist before any treatment or even one more vitamin or OTC drug.
watchful, active researcher and caregiver for stage IVb/c CC. surgeries 4/10 sigmoid etc & 5/11 para-aortic LN cluster; 8 yrs immuno-Chemo for mCRC; now no chemo
most of 2010 Life Extension recommendations and possibilities + more, some (much) higher, peaking ~2011-12, taper chemo to almost nothing mid 2018, IV C-->2021. Now supplements
most of 2010 Life Extension recommendations and possibilities + more, some (much) higher, peaking ~2011-12, taper chemo to almost nothing mid 2018, IV C-->2021. Now supplements
-
beach sunrise

- Posts: 1047
- Joined: Thu Mar 05, 2020 7:14 pm
Re: Checklists for newly diagnosed Stage IV patients?
Amen To That, Rp!
8/19 RC CEA 82.6 T3N0M0
5FU/rad 6 wk
IVC 75g 1 1/2 wks before surgery. Continue 2x a week
Surg 1/20 -margins T4bN1a IIIC G2 MSI- 1/20 LN+ LVI+ PNI-
pre cea 24 post 5.9
FOLFOX
7 rds 6-10 CEA 11.4 No more
CEA
7/20 11.1 8.8
8/20 7.8
9/20 8.8, 9, 8.6
10/20 8.1
11/20 8s
12/20 8s-9s
ADAPT++++ chrono
CEA
10/23/22 26.x
12/23/22 22.x
2023
1/5 17.1
1/20 15.9
3/30 14.9
6/12 13.3
8/1 2.1
Nodule RML SUV 1.3 5mm
Rolles 3 of 4 lung nodules cancer
KRAS
Chem-sens test failed Not enough ca cells to test
5FU/rad 6 wk
IVC 75g 1 1/2 wks before surgery. Continue 2x a week
Surg 1/20 -margins T4bN1a IIIC G2 MSI- 1/20 LN+ LVI+ PNI-
pre cea 24 post 5.9
FOLFOX
7 rds 6-10 CEA 11.4 No more
CEA
7/20 11.1 8.8
8/20 7.8
9/20 8.8, 9, 8.6
10/20 8.1
11/20 8s
12/20 8s-9s
ADAPT++++ chrono
CEA
10/23/22 26.x
12/23/22 22.x
2023
1/5 17.1
1/20 15.9
3/30 14.9
6/12 13.3
8/1 2.1
Nodule RML SUV 1.3 5mm
Rolles 3 of 4 lung nodules cancer
KRAS
Chem-sens test failed Not enough ca cells to test
Re: Checklists for newly diagnosed Stage IV patients?
I am curious as to what the “ more comprehensive blood data” is.
I did go back and look at Starbuck30 profile and what her fiancé posted. I’m still not sure what actually happened or why. Obviously her cancer must have been very aggressive. I didn’t see where her grade was posted. Isn’t the grade suppose to give an idea at how aggressive the cancer is? Honestly what happened to her is very scary.
I did go back and look at Starbuck30 profile and what her fiancé posted. I’m still not sure what actually happened or why. Obviously her cancer must have been very aggressive. I didn’t see where her grade was posted. Isn’t the grade suppose to give an idea at how aggressive the cancer is? Honestly what happened to her is very scary.
DH age 47
DX 10/22 stage 4
2 tumors in sigmoid colon 2 Mets liver
adenocarcinoma
MSI-H, TMB-H 38, KRAS G13V, ERBB2 neg, BRCA2, Lynch Syndrome
Grade 1 well differentiated
12/1/22 Yervoy and Opdivo CEA 5.4
12/19/22 Yervoy & Opdivo CEA 4.6
01/12/22 Yervoy & Opdivo CEA 3.9
2/13/23 Yervoy& Opdivo CEA 3.4
3/7/23 ct scans no change
3/9/23 Opdivo CEA 3.4
4/4/23 Opdivo CEA 2.3
6/1/23 Opdivo CEA 2.6
DX 10/22 stage 4
2 tumors in sigmoid colon 2 Mets liver
adenocarcinoma
MSI-H, TMB-H 38, KRAS G13V, ERBB2 neg, BRCA2, Lynch Syndrome
Grade 1 well differentiated
12/1/22 Yervoy and Opdivo CEA 5.4
12/19/22 Yervoy & Opdivo CEA 4.6
01/12/22 Yervoy & Opdivo CEA 3.9
2/13/23 Yervoy& Opdivo CEA 3.4
3/7/23 ct scans no change
3/9/23 Opdivo CEA 3.4
4/4/23 Opdivo CEA 2.3
6/1/23 Opdivo CEA 2.6
-
O Stoma Mia

- Posts: 1709
- Joined: Sat Jun 22, 2013 6:29 am
- Location: On vacation. Off-line for now.
Re: Checklists for newly diagnosed Stage IV patients?
nmorgen wrote:I am curious as to what the “ more comprehensive blood data” is...
More comprehensive blood data:
https://coloncancersupport.colonclub.com/viewtopic.php?f=1&t=53111&p=419599#p419695
https://coloncancersupport.colonclub.com/viewtopic.php?f=1&t=52100&p=407525#p407525
.
The difference between CMP and BMP
https://www.bassadvancedurgentcare.com/post/cmp-vs-bmp-heres-the-difference
.
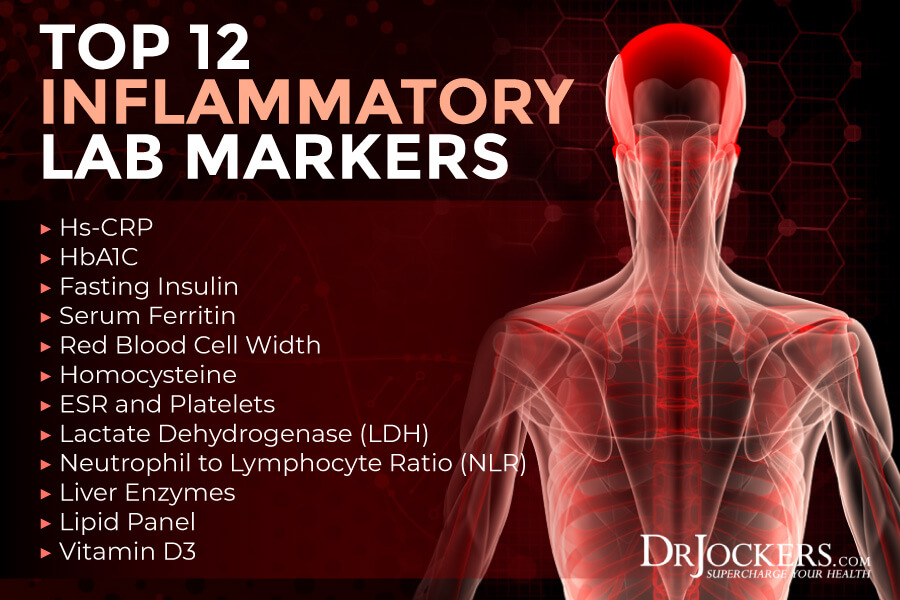
Ref: https://drjockers.com/inflammatory-lab-markers/
Return to “Colon Talk - Colon cancer (colorectal cancer) support forum”
Who is online
Users browsing this forum: Google [Bot] and 368 guests