Cancer aside, T2N0M0 means you caught it very early, which is great. The idea with early stage like that is it is still contained and can be removed wholesale.
My friend was T2N0M0 in 2014, had LAR no chemo, no radiation. She's been clear ever since. She does have occasional issues with scar tissue but has a normal life for the most part.
Getting a second opinion is a great idea. Scheduling in a large cancer center is always painful but be persistent. I can't speak as to the hysterectomy, only that my friend didn't have one.
I would recommend doing a genetic panel for the tumor, ideally also a ctDNA test post surgery. That'll give you peace of mind too. Do the genetic testing on either biopsy or post-op. The liquid biopsy reduces the reliability of the DNA test.
Good luck, your spouse and you are fortunate to have caught it so early.
New here, my spouse colonscopy likely. Scared.
Re: New here, my spouse colonscopy likely. Scared.
52M DX: RC lower rectum, guessing now 2cm from AV 4/27/2021
T3N0M0 adenocarcinoma with signet ring cell features
Tumor size 30mm
Tumor grade: G3
Baseline CEA 1.0
MSI status: MSS pMMR
Started Folfox 5/12/2021
Switched to FOLFIRINOX from session 2. 8 rounds total.
CT+MRI tumor contained shrunk 80%, no spread to other organs.
CRT started xeloda + 28 days Radiation 9/27-11/04
NED as of 4/06 CT/MRI/sigmoidoscopy
On W&W 04/06/2022
T3N0M0 adenocarcinoma with signet ring cell features
Tumor size 30mm
Tumor grade: G3
Baseline CEA 1.0
MSI status: MSS pMMR
Started Folfox 5/12/2021
Switched to FOLFIRINOX from session 2. 8 rounds total.
CT+MRI tumor contained shrunk 80%, no spread to other organs.
CRT started xeloda + 28 days Radiation 9/27-11/04
NED as of 4/06 CT/MRI/sigmoidoscopy
On W&W 04/06/2022
-
Nycomomohead
- Posts: 28
- Joined: Sat Oct 30, 2021 7:34 pm
Re: New here, my spouse colonscopy likely. Scared.
Thank you for your reply and advice. Praying for all of us.
Spouse, DX, 49F - Rectal Stage 1 - T2NOMO - 2CM - 7.8 from AV.
10.29.21 Rectal tumor 2cm, 10cm from AV | colonoscopy
11.01.21 Biospy - Malignant - adenocarcinoma
11.03.21 First consultation with Surgeon & Onc
11.04.21 CBC blood work looked good. CEA at 1.1
11.05.21 CT Scan. Good, no sign of spread. Precautionary Liver MRI scheduled.
11.09.21 MRI Pelvis. MRI Liver.
11.09.21 Staged as Stage 1. T2NOMO - 2CM - 7.8 from AV.
10.29.21 Rectal tumor 2cm, 10cm from AV | colonoscopy
11.01.21 Biospy - Malignant - adenocarcinoma
11.03.21 First consultation with Surgeon & Onc
11.04.21 CBC blood work looked good. CEA at 1.1
11.05.21 CT Scan. Good, no sign of spread. Precautionary Liver MRI scheduled.
11.09.21 MRI Pelvis. MRI Liver.
11.09.21 Staged as Stage 1. T2NOMO - 2CM - 7.8 from AV.
Re: New here, my spouse colonscopy likely. Scared.
To my knowledge, hysterectomy would only be under consideration if she has Lynch, or actual uterine cancer. Lynch cannot be diagnosed without genetic testing of both the tumor and her blood. I'd ask the doctor why he is recommending it.
I would definitely get a second opinion before undergoing a hysterectomy, even at 49.
ETA: apparently women who have BRAF may also be candidates for hysterectomy.
I would definitely get a second opinion before undergoing a hysterectomy, even at 49.
ETA: apparently women who have BRAF may also be candidates for hysterectomy.
F, 64 at DX CRC Stage IV
3/17/18 blockage, r hemi
11 of 25 LN,5 mesentery nodes
5mm liver met
pT3 pN2b pM1
BRAF wild, KRAS G12D
dMMR, MSI-H
5/18 FOLFOX
7/18 and 11/18 CT NED
12/18 MRI 5mm liver mass, 2 LNs in porta hepatis
12/31/18 Keytruda
6/19 Multiphasic CT LNs normal, Liver stable
6/28/19 Pause Key, predisone for joint pain
7/31/19 Restart Key
9/19 CT stable
Pain: all fails but Celebrex
12/23/19 CT stable
5/20 MRI stable/NED
6/20 Stop Key
All MRIs NED
3/17/18 blockage, r hemi
11 of 25 LN,5 mesentery nodes
5mm liver met
pT3 pN2b pM1
BRAF wild, KRAS G12D
dMMR, MSI-H
5/18 FOLFOX
7/18 and 11/18 CT NED
12/18 MRI 5mm liver mass, 2 LNs in porta hepatis
12/31/18 Keytruda
6/19 Multiphasic CT LNs normal, Liver stable
6/28/19 Pause Key, predisone for joint pain
7/31/19 Restart Key
9/19 CT stable
Pain: all fails but Celebrex
12/23/19 CT stable
5/20 MRI stable/NED
6/20 Stop Key
All MRIs NED
-
DarknessEmbraced
- Posts: 3817
- Joined: Sat Nov 01, 2014 4:54 pm
- Facebook Username: Riann Fletcher
- Location: New Brunswick, Canada
Re: New here, my spouse colonscopy likely. Scared.
I'm sorry for your wife's diagnosis and I hope her surgery goes well. *hugs*
Diagnosed 10/28/14, age 36
Colon Resection 11/20/14, LAR (no illeo)
Stage 2a colon cancer, T3NOMO
Lymph-vascular invasion undetermined
0/22 lymph nodes
No chemo, no radiation
Clear Colonoscopy 04/29/15
NED 10/20/15
Ischemic Colitis 01/21/16
NED 11/10/16
CT Scan moved up due to high CEA 08/21/17
NED 09/25/17
NED 12/21/18
Clear colonoscopy 09/23/19
Clear 5 year scans 11/21/19- Considered cured!
Colon Resection 11/20/14, LAR (no illeo)
Stage 2a colon cancer, T3NOMO
Lymph-vascular invasion undetermined
0/22 lymph nodes
No chemo, no radiation
Clear Colonoscopy 04/29/15
NED 10/20/15
Ischemic Colitis 01/21/16
NED 11/10/16
CT Scan moved up due to high CEA 08/21/17
NED 09/25/17
NED 12/21/18
Clear colonoscopy 09/23/19
Clear 5 year scans 11/21/19- Considered cured!
-
Nycomomohead
- Posts: 28
- Joined: Sat Oct 30, 2021 7:34 pm
Re: New here, my spouse colonscopy likely. Scared.
Thank you all for your thoughts and advice.
Spouse, DX, 49F - Rectal Stage 1 - T2NOMO - 2CM - 7.8 from AV.
10.29.21 Rectal tumor 2cm, 10cm from AV | colonoscopy
11.01.21 Biospy - Malignant - adenocarcinoma
11.03.21 First consultation with Surgeon & Onc
11.04.21 CBC blood work looked good. CEA at 1.1
11.05.21 CT Scan. Good, no sign of spread. Precautionary Liver MRI scheduled.
11.09.21 MRI Pelvis. MRI Liver.
11.09.21 Staged as Stage 1. T2NOMO - 2CM - 7.8 from AV.
10.29.21 Rectal tumor 2cm, 10cm from AV | colonoscopy
11.01.21 Biospy - Malignant - adenocarcinoma
11.03.21 First consultation with Surgeon & Onc
11.04.21 CBC blood work looked good. CEA at 1.1
11.05.21 CT Scan. Good, no sign of spread. Precautionary Liver MRI scheduled.
11.09.21 MRI Pelvis. MRI Liver.
11.09.21 Staged as Stage 1. T2NOMO - 2CM - 7.8 from AV.
-
Nycomomohead
- Posts: 28
- Joined: Sat Oct 30, 2021 7:34 pm
Re: New here, my spouse colonscopy likely. Scared.
My wife and I have decided on to go with the original surgeon after meeting with UPenn and MSK. MSK is extremely well run, but ultimately, all landed on the same treatment path. MSK did differ in offering robotic LAR, while the others would do non robotic LAR.
The original surgeon and team have been very responsive and timely and aligned with the 2nd opinions. Reference followups with doctors have all shown the surgeon to be skilled and caring.
My wife's surgery is about 1 week out. MSK said a temp ilestomy will be required. Our surgeon said it will be a surgery decision.
My wife is holding up well, but certain days are better than others. Stress and having the appetite to maintain her weight, lack of sleep are being experienced. Hot flashes from probable menopause also have her sleep and fatigue challenging.
Any tips for me to help my wife for what is ahead is always appreciated.
My thoughts are with all affected.
The original surgeon and team have been very responsive and timely and aligned with the 2nd opinions. Reference followups with doctors have all shown the surgeon to be skilled and caring.
My wife's surgery is about 1 week out. MSK said a temp ilestomy will be required. Our surgeon said it will be a surgery decision.
My wife is holding up well, but certain days are better than others. Stress and having the appetite to maintain her weight, lack of sleep are being experienced. Hot flashes from probable menopause also have her sleep and fatigue challenging.
Any tips for me to help my wife for what is ahead is always appreciated.
My thoughts are with all affected.
Last edited by Nycomomohead on Sun Nov 21, 2021 4:25 am, edited 1 time in total.
Spouse, DX, 49F - Rectal Stage 1 - T2NOMO - 2CM - 7.8 from AV.
10.29.21 Rectal tumor 2cm, 10cm from AV | colonoscopy
11.01.21 Biospy - Malignant - adenocarcinoma
11.03.21 First consultation with Surgeon & Onc
11.04.21 CBC blood work looked good. CEA at 1.1
11.05.21 CT Scan. Good, no sign of spread. Precautionary Liver MRI scheduled.
11.09.21 MRI Pelvis. MRI Liver.
11.09.21 Staged as Stage 1. T2NOMO - 2CM - 7.8 from AV.
10.29.21 Rectal tumor 2cm, 10cm from AV | colonoscopy
11.01.21 Biospy - Malignant - adenocarcinoma
11.03.21 First consultation with Surgeon & Onc
11.04.21 CBC blood work looked good. CEA at 1.1
11.05.21 CT Scan. Good, no sign of spread. Precautionary Liver MRI scheduled.
11.09.21 MRI Pelvis. MRI Liver.
11.09.21 Staged as Stage 1. T2NOMO - 2CM - 7.8 from AV.
Re: New here, my spouse colonscopy likely. Scared.
Nycomomohead wrote:My wife and I have decided on to go with the original surgeon after meeting with UPenn and MSK. MSK is extremely well run, but ultimately, all landed on the same treatment path. MSK did differ in offering robotic LAR, while the others would do non robotic LAR.
The original surgeon and team have been very responsive and timely and aligned with the 2nd opinions. Reference followups with doctors have all shown the surgeon to be skilled and caring.
My wife surgery is about 1 week out. MSK said a temp ilestomy will be required. Our surgeon said it will be a surgery decision.
My wife is holding up well, but certain days are better than others. Stress and having the appetite to maintain her weight, lack of sleep are being experienced. Hot flashes from probable menopause also have me sleep and fatigue challenging.
Any tips for me to help my wife for what is ahead is always appreciated.
My thoughts are with all affected.
It sounds like you are on a good path as far as treatment is concerned. I found meditation to be extremely helpful handling the emotional aspect. I was definitely a skeptic but am now a true believer. MSK has great videos on their website demonstrating meditation techniques.
5/19 IIIC sigmoid cancer 2/25 lymph nodes positive
5/19 surgery
7/19 FOLFOX 6 months
9/20 recurrence to single lymph node
10/20 FOLFIRI 5 rounds
1/21 surgery to remove lymph node
4/21 CT NED
8/21 CT NED
11/21 CT NED
2/22 CT NED
5/22 CT NED
8/22 PET NED
11/22 CT NED
3/23 PET lesion on liver
3/23 MRI confirmed lesion
4/23 liver surgery aborted lesion found on diaphragm
5/23 chemo started
7/23 CT shows shrinkage of lesion, consult scheduled with surgeon
5/19 surgery
7/19 FOLFOX 6 months
9/20 recurrence to single lymph node
10/20 FOLFIRI 5 rounds
1/21 surgery to remove lymph node
4/21 CT NED
8/21 CT NED
11/21 CT NED
2/22 CT NED
5/22 CT NED
8/22 PET NED
11/22 CT NED
3/23 PET lesion on liver
3/23 MRI confirmed lesion
4/23 liver surgery aborted lesion found on diaphragm
5/23 chemo started
7/23 CT shows shrinkage of lesion, consult scheduled with surgeon
-
Rock_Robster
- Posts: 1028
- Joined: Thu Oct 25, 2018 5:27 am
- Location: Brisbane, Australia
Re: New here, my spouse colonscopy likely. Scared.
I had a robotic ULAR with temporary ileostomy, reversed 6 months later.
As far as surgeries go it isn’t too bad, particularly if they do it minimally-invasively. But the adjustment for her system (both after surgery and after reversal) is substantial, and unfortunately you’re going through that at the same time as learning the skill set of managing an ostomy.
The goal is to get in and out of hospital as quickly as possible with the fewest complications. When she can leave hospital will be largely determined by: (1) pain can be managed with oral meds, (2) normal bowel movement has restarted, (3) any drains have slowed sufficiently or stopped, and (4) she can manage the ileostomy without nursing support.
(1) is usually not too bad for this type of surgery; thankfully. For (2) & (3) frequent, gentle walking is by far the best solution. Ask the hospital if they have an Enhanced Recovery After Surgery (ERAS) program, and if so follow it to the letter. If not, I can provide a link to a generic GI ERAS program and she can get onto it. The main thing is to resume very light walking and plain solid foods as quickly as possibly after surgery (ie within 24 hours), and then scale up to some pretty serious activity levels by discharge.
On (4), stoma care nurses are directly descended from one of the layers of heavenly choir angels, so make sure you meet with yours *before* the surgery (which will also involve marking a location for the stoma - she should wear her favourite jeans or whatever to this meeting so they can avoid the wasteband. For many folk, a higher stoma is easier than lower, as it can sit above the pants waistline). She should start doing her own bag changes etc. as soon as she is physically able, with nursing supervision. It will all be done on autopilot after about 3 weeks, but you’ve gotta get the muscle memory up. Matching the right stoma apparatuses to the person is also key; the stoma nurse can help a lot with this, but it’s not a bad idea to get in touch with the major providers too (Coloplast, Hollister, Convatec) and ask for some samples of their most popular products for new ileostomies. I was a big fan of the Coloplast Sensura Mio one-piece drainable bags, with the Coloplast Brava strips.
Breathing exercises are also important after surgery to avoid lung issues, I can post some tips on this if helpful (or you can Google these).
If she doesn’t have an ostomy, then recovering something close to normal bowel function is going to take some time. But perhaps we cross that bridge if we come to it, given a temporary ileostomy sounds more likely at this stage.
This is all about recovering quickly and getting home. There is another dimension to this which is that this is also *cancer* surgery, so maximising her oncological outcome and minimising recurrence risk is also crucial. Although she thankfully has a low-risk case, there are still measures that can taken that are also just good sense anyway. However there is a lot for you to take in here already, so if this is of interest let me know and I’ll post some more thoughts.
Good luck,
Rob
As far as surgeries go it isn’t too bad, particularly if they do it minimally-invasively. But the adjustment for her system (both after surgery and after reversal) is substantial, and unfortunately you’re going through that at the same time as learning the skill set of managing an ostomy.
The goal is to get in and out of hospital as quickly as possible with the fewest complications. When she can leave hospital will be largely determined by: (1) pain can be managed with oral meds, (2) normal bowel movement has restarted, (3) any drains have slowed sufficiently or stopped, and (4) she can manage the ileostomy without nursing support.
(1) is usually not too bad for this type of surgery; thankfully. For (2) & (3) frequent, gentle walking is by far the best solution. Ask the hospital if they have an Enhanced Recovery After Surgery (ERAS) program, and if so follow it to the letter. If not, I can provide a link to a generic GI ERAS program and she can get onto it. The main thing is to resume very light walking and plain solid foods as quickly as possibly after surgery (ie within 24 hours), and then scale up to some pretty serious activity levels by discharge.
On (4), stoma care nurses are directly descended from one of the layers of heavenly choir angels, so make sure you meet with yours *before* the surgery (which will also involve marking a location for the stoma - she should wear her favourite jeans or whatever to this meeting so they can avoid the wasteband. For many folk, a higher stoma is easier than lower, as it can sit above the pants waistline). She should start doing her own bag changes etc. as soon as she is physically able, with nursing supervision. It will all be done on autopilot after about 3 weeks, but you’ve gotta get the muscle memory up. Matching the right stoma apparatuses to the person is also key; the stoma nurse can help a lot with this, but it’s not a bad idea to get in touch with the major providers too (Coloplast, Hollister, Convatec) and ask for some samples of their most popular products for new ileostomies. I was a big fan of the Coloplast Sensura Mio one-piece drainable bags, with the Coloplast Brava strips.
Breathing exercises are also important after surgery to avoid lung issues, I can post some tips on this if helpful (or you can Google these).
If she doesn’t have an ostomy, then recovering something close to normal bowel function is going to take some time. But perhaps we cross that bridge if we come to it, given a temporary ileostomy sounds more likely at this stage.
This is all about recovering quickly and getting home. There is another dimension to this which is that this is also *cancer* surgery, so maximising her oncological outcome and minimising recurrence risk is also crucial. Although she thankfully has a low-risk case, there are still measures that can taken that are also just good sense anyway. However there is a lot for you to take in here already, so if this is of interest let me know and I’ll post some more thoughts.
Good luck,
Rob
41M Australia
2018 Dx RC
G2 EMVI LVI, 4 liver mets
pT3N1aM1a Stage IVa MSS NRAS G13R
CEA 14>2>32>16>19>30>140>70
11/18 FOLFOX
3/19 Liver resection
5/19 Pelvic IMRT
7/19 ULAR
8/19 Liver met
8/19 FOLFOX, FOLFOXIRI, FOLFIRI
12/19 Liver resection
NED 2 years
11/21 Liver met, PALN, lung nodules
3/22 PVE, lymphadenectomy, liver SBRT
10/22 PALN SBRT
11/22 Liver mets, peri nodule. Xeloda+Bev
4/23 XELIRI+Bev
9/23 ATRIUM trial
12/23 Modified FOLFIRI+Bev
3/24 VAXINIA (CF33 + hNIS) trial
2018 Dx RC
G2 EMVI LVI, 4 liver mets
pT3N1aM1a Stage IVa MSS NRAS G13R
CEA 14>2>32>16>19>30>140>70
11/18 FOLFOX
3/19 Liver resection
5/19 Pelvic IMRT
7/19 ULAR
8/19 Liver met
8/19 FOLFOX, FOLFOXIRI, FOLFIRI
12/19 Liver resection
NED 2 years
11/21 Liver met, PALN, lung nodules
3/22 PVE, lymphadenectomy, liver SBRT
10/22 PALN SBRT
11/22 Liver mets, peri nodule. Xeloda+Bev
4/23 XELIRI+Bev
9/23 ATRIUM trial
12/23 Modified FOLFIRI+Bev
3/24 VAXINIA (CF33 + hNIS) trial

Re: New here, my spouse colonscopy likely. Scared.
Nycomomohead wrote:... Any tips for me to help my wife for what is ahead is always appreciated...
In preparation for the up-coming LAR surgery, I think it would be a good idea to do some advance research on ostomy support, under the assumption that a temporary ileostomy might be required.
There are several things you can do to help your wife prepare for this in advance, should it become necessary for the surgeon to create a temporary ileostomy.
1~~ Placement of the ostomy. Before the LAR, the surgeon will probably place an indelible mark on the abdomen at the location where he/she intends to make the incision. It is very important to make the incision at a place that will not cause problems with the ostomy device later on. In particular, the incision point should be in a relatively flat part of the right abdomen so that ostomy devices can be easily attached and detached, and so that the device is not installed in a natural fold in the abdomen skin. Location is also important so that the ostomy device is not in a location where a seatbelt strap will squash the ostomy bag when a seatbelt is fastened. If the incision is in an awkward place, then there could be constant problems with the ostomy bag springing leaks and causing a mess.
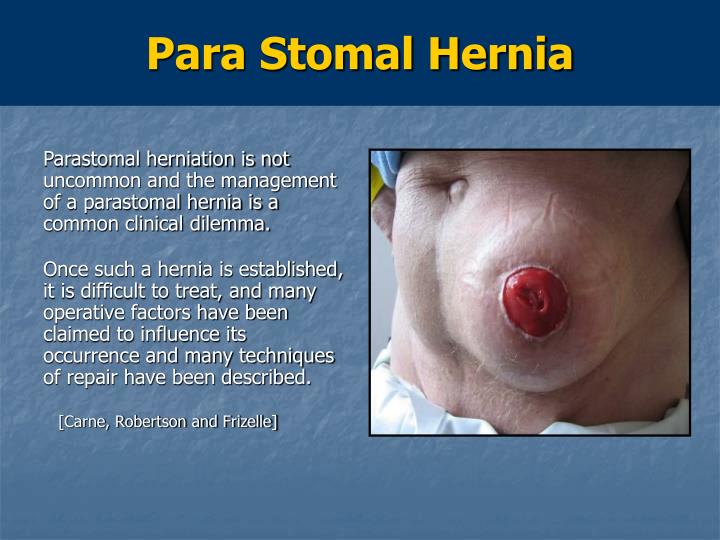
2~~ WOCN nurse. It is important to find and make an appointment with an experienced Wound Ostomy Continence Nurse (WOCN) to get advice on the best type of ostomy to use, and to get training on how to change ostomy devices when they need to be changed. There is also a need to get preventive education and training to avoid a parastomal hernia and avoid the need for a future hernia repair operation. Parastomal hernias are a big nuisance and should be avoided at all cost.
{kind=link}
3~~ Post-surgery precautions. There are various recommendations about what to do, and what not to do, just after surgery so as to maximize recovery and minimize post-surgery complications. Read and re-read Rock_Robster's post because it contains excellent advice in this regard.
4~~ Ostomy support forum. I think it would be a good idea to have a look at the ostomy.org website to see what kind of support they have to offer, and to see if you might want to register for their support forum.
That's all for now. Good luck !
-
Nycomomohead
- Posts: 28
- Joined: Sat Oct 30, 2021 7:34 pm
Re: New here, my spouse colonscopy likely. Scared.
Thanks everyone for your caring responses.
They have said they will do a minimally invasive LAR and showed where the incisions will be. My wife had 2 c-sections, so, she feels she is prepped on that end.
Thank you for the reinforcement on walking. The hospital did advise us they follow an ERAS program and gave us materials on it.
On the appointment for the sign off on surgery, we also did a marking placement for the potential ilestomy. You are so right about the placement higher potential being preferable. They gave 2 versions, a single and a double stoma.
My wife tried the single piece, and trialed the lower spot. It ended up bothering her as she sat. She has not really worn it, I will let her know to try on the higher spot.
The nurse also advised doing research on ilestomy bags on Hollister. I was stunned at the amount of choices. I will ask for samples.
Thank you for the advise on Coloplast.
Finally, some other notes.
MSK said 3 to 4 days for release, with here going with 4 to 5.
We also are doing genetics on a number of cancers, but with a primary focus on colon and stomach. The biopsy of the tumor from the colonscopy did not show Lynch or other mutations per the surgeon, so we also opted not to do a hysterectomy.
Finally, both the MSK and original doctor via their sigmoidoscopies said they measure the tumor at 7cm from the AV.
They have said they will do a minimally invasive LAR and showed where the incisions will be. My wife had 2 c-sections, so, she feels she is prepped on that end.
Thank you for the reinforcement on walking. The hospital did advise us they follow an ERAS program and gave us materials on it.
On the appointment for the sign off on surgery, we also did a marking placement for the potential ilestomy. You are so right about the placement higher potential being preferable. They gave 2 versions, a single and a double stoma.
My wife tried the single piece, and trialed the lower spot. It ended up bothering her as she sat. She has not really worn it, I will let her know to try on the higher spot.
The nurse also advised doing research on ilestomy bags on Hollister. I was stunned at the amount of choices. I will ask for samples.
Thank you for the advise on Coloplast.
Finally, some other notes.
MSK said 3 to 4 days for release, with here going with 4 to 5.
We also are doing genetics on a number of cancers, but with a primary focus on colon and stomach. The biopsy of the tumor from the colonscopy did not show Lynch or other mutations per the surgeon, so we also opted not to do a hysterectomy.
Finally, both the MSK and original doctor via their sigmoidoscopies said they measure the tumor at 7cm from the AV.
Rock_Robster wrote:I had a robotic ULAR with temporary ileostomy, reversed 6 months later.
As far as surgeries go it isn’t too bad, particularly if they do it minimally-invasively. But the adjustment for her system (both after surgery and after reversal) is substantial, and unfortunately you’re going through that at the same time as learning the skill set of managing an ostomy.
The goal is to get in and out of hospital as quickly as possible with the fewest complications. When she can leave hospital will be largely determined by: (1) pain can be managed with oral meds, (2) normal bowel movement has restarted, (3) any drains have slowed sufficiently or stopped, and (4) she can manage the ileostomy without nursing support.
(1) is usually not too bad for this type of surgery; thankfully. For (2) & (3) frequent, gentle walking is by far the best solution. Ask the hospital if they have an Enhanced Recovery After Surgery (ERAS) program, and if so follow it to the letter. If not, I can provide a link to a generic GI ERAS program and she can get onto it. The main thing is to resume very light walking and plain solid foods as quickly as possibly after surgery (ie within 24 hours), and then scale up to some pretty serious activity levels by discharge.
On (4), stoma care nurses are directly descended from one of the layers of heavenly choir angels, so make sure you meet with yours *before* the surgery (which will also involve marking a location for the stoma - she should wear her favourite jeans or whatever to this meeting so they can avoid the wasteband. For many folk, a higher stoma is easier than lower, as it can sit above the pants waistline). She should start doing her own bag changes etc. as soon as she is physically able, with nursing supervision. It will all be done on autopilot after about 3 weeks, but you’ve gotta get the muscle memory up. Matching the right stoma apparatuses to the person is also key; the stoma nurse can help a lot with this, but it’s not a bad idea to get in touch with the major providers too (Coloplast, Hollister, Convatec) and ask for some samples of their most popular products for new ileostomies. I was a big fan of the Coloplast Sensura Mio one-piece drainable bags, with the Coloplast Brava strips.
Breathing exercises are also important after surgery to avoid lung issues, I can post some tips on this if helpful (or you can Google these).
If she doesn’t have an ostomy, then recovering something close to normal bowel function is going to take some time. But perhaps we cross that bridge if we come to it, given a temporary ileostomy sounds more likely at this stage.
This is all about recovering quickly and getting home. There is another dimension to this which is that this is also *cancer* surgery, so maximising her oncological outcome and minimising recurrence risk is also crucial. Although she thankfully has a low-risk case, there are still measures that can taken that are also just good sense anyway. However there is a lot for you to take in here already, so if this is of interest let me know and I’ll post some more thoughts.
Good luck,
Rob
Spouse, DX, 49F - Rectal Stage 1 - T2NOMO - 2CM - 7.8 from AV.
10.29.21 Rectal tumor 2cm, 10cm from AV | colonoscopy
11.01.21 Biospy - Malignant - adenocarcinoma
11.03.21 First consultation with Surgeon & Onc
11.04.21 CBC blood work looked good. CEA at 1.1
11.05.21 CT Scan. Good, no sign of spread. Precautionary Liver MRI scheduled.
11.09.21 MRI Pelvis. MRI Liver.
11.09.21 Staged as Stage 1. T2NOMO - 2CM - 7.8 from AV.
10.29.21 Rectal tumor 2cm, 10cm from AV | colonoscopy
11.01.21 Biospy - Malignant - adenocarcinoma
11.03.21 First consultation with Surgeon & Onc
11.04.21 CBC blood work looked good. CEA at 1.1
11.05.21 CT Scan. Good, no sign of spread. Precautionary Liver MRI scheduled.
11.09.21 MRI Pelvis. MRI Liver.
11.09.21 Staged as Stage 1. T2NOMO - 2CM - 7.8 from AV.
-
Nycomomohead
- Posts: 28
- Joined: Sat Oct 30, 2021 7:34 pm
Re: New here, my spouse colonscopy likely. Scared.
Rob, you mentioned maximizing this surgery to avoid reoccurence. This is paramount to us. LARS has been on our mind, but also we worry about the risk of reoccurence and how best to avoid it.
Can you share your thoughts? We are praying that post surgery, nothing changes from a stage 1 diagnosis. Reading through materials and confirming with both Docs.
Stage 1 standard of care does not call for chemo or radiation post surgery.
I have been focusing on is doing what I can to do maximize monitoring. So I am going to discuss with Oncologist, options including Signatare. Open questions I have are how often I should ask for CEA bloodshed, along with what is the right frequency for colonscopies post.
This has also given me a wakeup call on my health, and I have scheduled a Urologist appointment to check my prostate. No bigger wakeup on the need to do what you can to prevent illness.
Also, been reading so many differing views on diet post surgery. I have modified our diets, to in general, cut out processed foods and sweets. Reading up use of different foods and aides dependent on loose stools or constipation.
A lot to take in.
Thank you for the below. I will follow up on who the nurse will be. The surgical team nurse that surgeon had us meet with did the stoma walk through and marking. She indicated that a in home nurse would be provided if stoma was required to help, if needed.
As the Doc still has said this is a surgery call, I didn't want to push to much on the stoma, but will review further.
They noted, on average, 6 weeks for temp stoma.
quote="JJH"]
In preparation for the up-coming LAR surgery, I think it would be a good idea to do some advance research on ostomy support, under the assumption that a temporary ileostomy might be required.
There are several things you can do to help your wife prepare for this in advance, should it become necessary for the surgeon to create a temporary ileostomy.
1~~ Placement of the ostomy. Before the LAR, the surgeon will probably place an indelible mark on the abdomen at the location where he/she intends to make the incision. It is very important to make the incision at a place that will not cause problems with the ostomy device later on. In particular, the incision point should be in a relatively flat part of the right abdomen so that ostomy devices can be easily attached and detached, and so that the device is not installed in a natural fold in the abdomen skin. Location is also important so that the ostomy device is not in a location where a seatbelt strap will squash the ostomy bag when a seatbelt is fastened. If the incision is in an awkward place, then there could be constant problems with the ostomy bag springing leaks and causing a mess.
2~~ WOCN nurse. It is important to find and make an appointment with an experienced Wound Ostomy Continence Nurse (WOCN) to get advice on the best type of ostomy to use, and to get training on how to change ostomy devices when they need to be changed. There is also a need to get preventive education and training to avoid a parastomal hernia and avoid the need for a future hernia repair operation. Parastomal hernias are a big nuisance and should be avoided at all cost.
3~~ Post-surgery precautions. There are various recommendations about what to do, and what not to do, just after surgery so as to maximize recovery and minimize post-surgery complications. Read and re-read Rock_Robster's post because it contains excellent advice in this regard.
4~~ Ostomy support forum. I think it would be a good idea to have a look at the ostomy.org website to see what kind of support they have to offer, and to see if you might want to register for their support forum.
That's all for now. Good luck ![/quote]
Can you share your thoughts? We are praying that post surgery, nothing changes from a stage 1 diagnosis. Reading through materials and confirming with both Docs.
Stage 1 standard of care does not call for chemo or radiation post surgery.
I have been focusing on is doing what I can to do maximize monitoring. So I am going to discuss with Oncologist, options including Signatare. Open questions I have are how often I should ask for CEA bloodshed, along with what is the right frequency for colonscopies post.
This has also given me a wakeup call on my health, and I have scheduled a Urologist appointment to check my prostate. No bigger wakeup on the need to do what you can to prevent illness.
Also, been reading so many differing views on diet post surgery. I have modified our diets, to in general, cut out processed foods and sweets. Reading up use of different foods and aides dependent on loose stools or constipation.
A lot to take in.
Thank you for the below. I will follow up on who the nurse will be. The surgical team nurse that surgeon had us meet with did the stoma walk through and marking. She indicated that a in home nurse would be provided if stoma was required to help, if needed.
As the Doc still has said this is a surgery call, I didn't want to push to much on the stoma, but will review further.
They noted, on average, 6 weeks for temp stoma.
quote="JJH"]
Nycomomohead wrote:... Any tips for me to help my wife for what is ahead is always appreciated...
In preparation for the up-coming LAR surgery, I think it would be a good idea to do some advance research on ostomy support, under the assumption that a temporary ileostomy might be required.
There are several things you can do to help your wife prepare for this in advance, should it become necessary for the surgeon to create a temporary ileostomy.
1~~ Placement of the ostomy. Before the LAR, the surgeon will probably place an indelible mark on the abdomen at the location where he/she intends to make the incision. It is very important to make the incision at a place that will not cause problems with the ostomy device later on. In particular, the incision point should be in a relatively flat part of the right abdomen so that ostomy devices can be easily attached and detached, and so that the device is not installed in a natural fold in the abdomen skin. Location is also important so that the ostomy device is not in a location where a seatbelt strap will squash the ostomy bag when a seatbelt is fastened. If the incision is in an awkward place, then there could be constant problems with the ostomy bag springing leaks and causing a mess.
2~~ WOCN nurse. It is important to find and make an appointment with an experienced Wound Ostomy Continence Nurse (WOCN) to get advice on the best type of ostomy to use, and to get training on how to change ostomy devices when they need to be changed. There is also a need to get preventive education and training to avoid a parastomal hernia and avoid the need for a future hernia repair operation. Parastomal hernias are a big nuisance and should be avoided at all cost.
3~~ Post-surgery precautions. There are various recommendations about what to do, and what not to do, just after surgery so as to maximize recovery and minimize post-surgery complications. Read and re-read Rock_Robster's post because it contains excellent advice in this regard.
4~~ Ostomy support forum. I think it would be a good idea to have a look at the ostomy.org website to see what kind of support they have to offer, and to see if you might want to register for their support forum.
That's all for now. Good luck ![/quote]
Last edited by Nycomomohead on Sun Nov 21, 2021 5:10 am, edited 1 time in total.
Spouse, DX, 49F - Rectal Stage 1 - T2NOMO - 2CM - 7.8 from AV.
10.29.21 Rectal tumor 2cm, 10cm from AV | colonoscopy
11.01.21 Biospy - Malignant - adenocarcinoma
11.03.21 First consultation with Surgeon & Onc
11.04.21 CBC blood work looked good. CEA at 1.1
11.05.21 CT Scan. Good, no sign of spread. Precautionary Liver MRI scheduled.
11.09.21 MRI Pelvis. MRI Liver.
11.09.21 Staged as Stage 1. T2NOMO - 2CM - 7.8 from AV.
10.29.21 Rectal tumor 2cm, 10cm from AV | colonoscopy
11.01.21 Biospy - Malignant - adenocarcinoma
11.03.21 First consultation with Surgeon & Onc
11.04.21 CBC blood work looked good. CEA at 1.1
11.05.21 CT Scan. Good, no sign of spread. Precautionary Liver MRI scheduled.
11.09.21 MRI Pelvis. MRI Liver.
11.09.21 Staged as Stage 1. T2NOMO - 2CM - 7.8 from AV.
-
Nycomomohead
- Posts: 28
- Joined: Sat Oct 30, 2021 7:34 pm
Re: New here, my spouse colonscopy likely. Scared.
[
Thank you, my brother did share with me mediation has been helpful for 2 friends who are battling different cancers.
You are so right on MSK, they have wonderful materials.
quote="Dennyp"]
It sounds like you are on a good path as far as treatment is concerned. I found meditation to be extremely helpful handling the emotional aspect. I was definitely a skeptic but am now a true believer. MSK has great videos on their website demonstrating meditation techniques.[/quote]
Thank you, my brother did share with me mediation has been helpful for 2 friends who are battling different cancers.
You are so right on MSK, they have wonderful materials.
quote="Dennyp"]
Nycomomohead wrote:My wife and I have decided on to go with the original surgeon after meeting with UPenn and MSK. MSK is extremely well run, but ultimately, all landed on the same treatment path. MSK did differ in offering robotic LAR, while the others would do non robotic LAR.
The original surgeon and team have been very responsive and timely and aligned with the 2nd opinions. Reference followups with doctors have all shown the surgeon to be skilled and caring.
My wife surgery is about 1 week out. MSK said a temp ilestomy will be required. Our surgeon said it will be a surgery decision.
My wife is holding up well, but certain days are better than others. Stress and having the appetite to maintain her weight, lack of sleep are being experienced. Hot flashes from probable menopause also have me sleep and fatigue challenging.
Any tips for me to help my wife for what is ahead is always appreciated.
My thoughts are with all affected.
It sounds like you are on a good path as far as treatment is concerned. I found meditation to be extremely helpful handling the emotional aspect. I was definitely a skeptic but am now a true believer. MSK has great videos on their website demonstrating meditation techniques.[/quote]
Spouse, DX, 49F - Rectal Stage 1 - T2NOMO - 2CM - 7.8 from AV.
10.29.21 Rectal tumor 2cm, 10cm from AV | colonoscopy
11.01.21 Biospy - Malignant - adenocarcinoma
11.03.21 First consultation with Surgeon & Onc
11.04.21 CBC blood work looked good. CEA at 1.1
11.05.21 CT Scan. Good, no sign of spread. Precautionary Liver MRI scheduled.
11.09.21 MRI Pelvis. MRI Liver.
11.09.21 Staged as Stage 1. T2NOMO - 2CM - 7.8 from AV.
10.29.21 Rectal tumor 2cm, 10cm from AV | colonoscopy
11.01.21 Biospy - Malignant - adenocarcinoma
11.03.21 First consultation with Surgeon & Onc
11.04.21 CBC blood work looked good. CEA at 1.1
11.05.21 CT Scan. Good, no sign of spread. Precautionary Liver MRI scheduled.
11.09.21 MRI Pelvis. MRI Liver.
11.09.21 Staged as Stage 1. T2NOMO - 2CM - 7.8 from AV.
O/T: PSA test
Nycomomohead wrote:... This has also given me a wakeup call on my health, and I have scheduled a Urologist appointment to check my prostate...
O Stoma Mia wrote:... Male patients above a certain age should be sure to have a Prostate Specific Antigen (PSA) prostate test annually to check on two things: (1) if the PSA value has gone out of normal range, and (2) if the value has more than doubled in the previous year. If so, then it is time to schedule an appointment with a urologist to see if the current elevation is something to worry about.
According to current literature, the best non-invasive test for checking on prostate cancer is a specialized multi-parameter MRI scan called mpMRI. This kind of scan is designed to look specifically for abnormal blood flow in the prostate, which would be indicative of an emergent cancer. If it is caught early enough, then this would be before the cancer has had a chance to metastasize to the bones. In prostate cancer, metastasis to the bones is generally the first, and primary metastasis site. Other metastases come later.
You can read about it in this primer:
A PROSTATE CANCER PRIMER
https://prostatecancer2020vision.org/wp-content/uploads/2020/12/ProstatePrimer_V3.pdf
Website: https://prostatecancer2020vision.org
-
Rock_Robster
- Posts: 1028
- Joined: Thu Oct 25, 2018 5:27 am
- Location: Brisbane, Australia
Re: New here, my spouse colonscopy likely. Scared.
So you’re right to point out that this is low risk, and there’s a very high likelihood you will both get through this and never have to face cancer again. Chemo and radiation both have serious, potentially permanent side effects - so you would only want to do them if there is strong evidence of benefit.
So, here’s my thoughts on having as good a cancer surgery outcome as possible, summarised from reading and experience. Most big cancer hospitals do 95% of this stuff anyway as standard. At general hospitals, you may have to take the lead on some of it a bit more.
The most important person in all of this is actually the anaesthetist. You should have a pre-anaesthesia consultation with them before this surgery - this is the time to bring this stuff up, and agree the plan.
GENERAL AIMS:
- Start strong
- Manage pain appropriately
- Mobilise early and often
- Minimise inflammatory response
- Minimise immunosuppression
- Heal fast (minimise angiogenesis)
BEFORE SURGERY
- Zero alcohol or cigarettes between now and surgery.
- Surgery should ideally be done laparoscopically
- Do not go into surgery in an unnecessarily weak and fasted state. Some fasting is probably required, but ask the anaesthetist if you can do a 6-hour fast, with clear liquids allowed prior to that. If so, make clear soups or buy bone broth and drink this up until 6 hours beforehand. Make sure you have some calories on the day of surgery.
- Ask the anaesthetist if you can have a small clear carbohydrate drink 2 hours before surgery. This should also be fine. There is a product called ‘DEX’ that is made for this; otherwise a something like Ensure Clear or even clear Gatorade is better than nothing.
PAIN MANAGEMENT
- Proper pain control is absolute essential to avoid a systemic stress response to trauma.
- Ask the anaesthetist about regional pain relief - such as a spinal (intrathecal) block or epidural before surgery, and a local anaesthetic infusion (aka “pain buster”) if there’s going to be a large wound. This reduces the trauma response during surgery and means less systemic pain meds are required. Spinal blocks often use morphine, but you can also ask for a slow-release fentanyl solution instead (which I had - worked well).
- Volatile gases should not be used for anaesthesia during cancer surgery. Tell your anaesthetist you want “total IV anaesthesia” if it is clinically safe to do so. Refer them to the VAPOR-C trial if they want more background on this.
- Opioids will be necessary, however these are also immunosuppressive. Morphine is the worst and should be completely avoided (it really has no role in surgery now). Oxycodone is better but still suppressive. Tramadol is ideal as it is actually immunomodulatory, but may not be strong enough by itself. Fentanyl is a good compromise, but short-acting which means it’s good for patient-controlled analgesia. My solution was to use IV Tramadol or ketamine (non-opioid), with a Fentanyl push-button top-up as needed (PCA). I could then take the IV down after a few days and switch to oral Tramadol only. However if this isn’t enough, add more pain relief - do not tolerate pain for the sake of immunity as it will just be counterproductive.
- Keeping inflammation low after surgery is important. Ask the anaesthetist to order a low dose oral anti-inflammatory - Celebrex is ideal (as a COX-2 inhibitor) - for 1-2 weeks after surgery. This reduces systemic inflammation and makes other painkillers more effective, without adding bleeding risk.
- Good sleep is essential. If you have trouble sleeping in hospital (as I do), ask for a low dose (0.5-1.0mg) of Ativan for nighttime. At this dose and for less than a week, dependency risk is very low.
AFTER SURGERY
- As soon as you can tolerate it without nausea/vomiting, start eating soft foods. This should ideally be within 24 hours. Small meals frequently is better. Ask for IV or oral ondansetron (Zofran) to avoid nausea after eating if needed.
- Drains and catheters should be removed as soon as possible (catheters within 48 hours). Ask the surgeon at what output volume they would be happy to remove the drain, and make sure the nurses check this regularly (at least daily) to see if they can come out.
- Ask the nurses the distance of one lap of the ward (or count the steps yourself). Ideal activity level is the below (I didn’t quite manage this...):
- 1000 steps 24 hours after surgery
- 4000 steps per day after 2-3 days
- 8000 steps per day by discharge
- The key is to do small amounts, frequently. Doing these in one go will be impossible, so perhaps break this over 4-5 short sessions per day.
- It is critical that you have enough pain meds to be able to walk. If you can’t walk without intolerable pain, then talk to the surgeon, anaesthetist or pain team about reviewing the pain protocol. Early mobility is essential.
- Move out of bed as early as possible. Start by having meals in the chair, then progress to spending the days mostly in the chair, and only using the bed for naps or sleeping.
- Look up post-surgery breathing exercises online and do these regularly (ideally hourly, but at least 5-6 times per day) to help restore lung capacity quickly and avoid complications. Buying a spirometer can help make it more visible and interesting.
So, here’s my thoughts on having as good a cancer surgery outcome as possible, summarised from reading and experience. Most big cancer hospitals do 95% of this stuff anyway as standard. At general hospitals, you may have to take the lead on some of it a bit more.
The most important person in all of this is actually the anaesthetist. You should have a pre-anaesthesia consultation with them before this surgery - this is the time to bring this stuff up, and agree the plan.
GENERAL AIMS:
- Start strong
- Manage pain appropriately
- Mobilise early and often
- Minimise inflammatory response
- Minimise immunosuppression
- Heal fast (minimise angiogenesis)
BEFORE SURGERY
- Zero alcohol or cigarettes between now and surgery.
- Surgery should ideally be done laparoscopically
- Do not go into surgery in an unnecessarily weak and fasted state. Some fasting is probably required, but ask the anaesthetist if you can do a 6-hour fast, with clear liquids allowed prior to that. If so, make clear soups or buy bone broth and drink this up until 6 hours beforehand. Make sure you have some calories on the day of surgery.
- Ask the anaesthetist if you can have a small clear carbohydrate drink 2 hours before surgery. This should also be fine. There is a product called ‘DEX’ that is made for this; otherwise a something like Ensure Clear or even clear Gatorade is better than nothing.
PAIN MANAGEMENT
- Proper pain control is absolute essential to avoid a systemic stress response to trauma.
- Ask the anaesthetist about regional pain relief - such as a spinal (intrathecal) block or epidural before surgery, and a local anaesthetic infusion (aka “pain buster”) if there’s going to be a large wound. This reduces the trauma response during surgery and means less systemic pain meds are required. Spinal blocks often use morphine, but you can also ask for a slow-release fentanyl solution instead (which I had - worked well).
- Volatile gases should not be used for anaesthesia during cancer surgery. Tell your anaesthetist you want “total IV anaesthesia” if it is clinically safe to do so. Refer them to the VAPOR-C trial if they want more background on this.
- Opioids will be necessary, however these are also immunosuppressive. Morphine is the worst and should be completely avoided (it really has no role in surgery now). Oxycodone is better but still suppressive. Tramadol is ideal as it is actually immunomodulatory, but may not be strong enough by itself. Fentanyl is a good compromise, but short-acting which means it’s good for patient-controlled analgesia. My solution was to use IV Tramadol or ketamine (non-opioid), with a Fentanyl push-button top-up as needed (PCA). I could then take the IV down after a few days and switch to oral Tramadol only. However if this isn’t enough, add more pain relief - do not tolerate pain for the sake of immunity as it will just be counterproductive.
- Keeping inflammation low after surgery is important. Ask the anaesthetist to order a low dose oral anti-inflammatory - Celebrex is ideal (as a COX-2 inhibitor) - for 1-2 weeks after surgery. This reduces systemic inflammation and makes other painkillers more effective, without adding bleeding risk.
- Good sleep is essential. If you have trouble sleeping in hospital (as I do), ask for a low dose (0.5-1.0mg) of Ativan for nighttime. At this dose and for less than a week, dependency risk is very low.
AFTER SURGERY
- As soon as you can tolerate it without nausea/vomiting, start eating soft foods. This should ideally be within 24 hours. Small meals frequently is better. Ask for IV or oral ondansetron (Zofran) to avoid nausea after eating if needed.
- Drains and catheters should be removed as soon as possible (catheters within 48 hours). Ask the surgeon at what output volume they would be happy to remove the drain, and make sure the nurses check this regularly (at least daily) to see if they can come out.
- Ask the nurses the distance of one lap of the ward (or count the steps yourself). Ideal activity level is the below (I didn’t quite manage this...):
- 1000 steps 24 hours after surgery
- 4000 steps per day after 2-3 days
- 8000 steps per day by discharge
- The key is to do small amounts, frequently. Doing these in one go will be impossible, so perhaps break this over 4-5 short sessions per day.
- It is critical that you have enough pain meds to be able to walk. If you can’t walk without intolerable pain, then talk to the surgeon, anaesthetist or pain team about reviewing the pain protocol. Early mobility is essential.
- Move out of bed as early as possible. Start by having meals in the chair, then progress to spending the days mostly in the chair, and only using the bed for naps or sleeping.
- Look up post-surgery breathing exercises online and do these regularly (ideally hourly, but at least 5-6 times per day) to help restore lung capacity quickly and avoid complications. Buying a spirometer can help make it more visible and interesting.
41M Australia
2018 Dx RC
G2 EMVI LVI, 4 liver mets
pT3N1aM1a Stage IVa MSS NRAS G13R
CEA 14>2>32>16>19>30>140>70
11/18 FOLFOX
3/19 Liver resection
5/19 Pelvic IMRT
7/19 ULAR
8/19 Liver met
8/19 FOLFOX, FOLFOXIRI, FOLFIRI
12/19 Liver resection
NED 2 years
11/21 Liver met, PALN, lung nodules
3/22 PVE, lymphadenectomy, liver SBRT
10/22 PALN SBRT
11/22 Liver mets, peri nodule. Xeloda+Bev
4/23 XELIRI+Bev
9/23 ATRIUM trial
12/23 Modified FOLFIRI+Bev
3/24 VAXINIA (CF33 + hNIS) trial
2018 Dx RC
G2 EMVI LVI, 4 liver mets
pT3N1aM1a Stage IVa MSS NRAS G13R
CEA 14>2>32>16>19>30>140>70
11/18 FOLFOX
3/19 Liver resection
5/19 Pelvic IMRT
7/19 ULAR
8/19 Liver met
8/19 FOLFOX, FOLFOXIRI, FOLFIRI
12/19 Liver resection
NED 2 years
11/21 Liver met, PALN, lung nodules
3/22 PVE, lymphadenectomy, liver SBRT
10/22 PALN SBRT
11/22 Liver mets, peri nodule. Xeloda+Bev
4/23 XELIRI+Bev
9/23 ATRIUM trial
12/23 Modified FOLFIRI+Bev
3/24 VAXINIA (CF33 + hNIS) trial
-
Rock_Robster
- Posts: 1028
- Joined: Thu Oct 25, 2018 5:27 am
- Location: Brisbane, Australia
Re: New here, my spouse colonscopy likely. Scared.
One more side comment - I bought one of the below and it literally changed the game for having an ostomy. I swear I wore it 24/7 and only took it off to shower (I used a waterproof bag shower cover so I didn’t have to blow-dry the bag). I would even just loosen the belt to sleep in it. It provides support and prevents the weight of the bag from hanging on the adhesive, and also keeps things discrete so if anything pokes out, all that shows is black neoprene fabric. Not cheap as each one is custom made, but worth every cent. For an ileo go for the “stingray” version of the Stealth Belt Pro so it stays vertical.
http://www.stealthbelt.com
PS: I do not get paid by Stealth Belt, but after my stoma nurse saw it I know they’re selling a lot more!!
PPS: let’s get through the surgery and home first, then we can discuss diet, LARS, surveillance, survivorship etc. There is however one fantastic resource from the Australian government I’d highly recommend reading about managing digestion after GI surgery - particularly relevant post-reversal: https://coastcolorectal.com.au/wp-conte ... urgery.pdf
http://www.stealthbelt.com
PS: I do not get paid by Stealth Belt, but after my stoma nurse saw it I know they’re selling a lot more!!
PPS: let’s get through the surgery and home first, then we can discuss diet, LARS, surveillance, survivorship etc. There is however one fantastic resource from the Australian government I’d highly recommend reading about managing digestion after GI surgery - particularly relevant post-reversal: https://coastcolorectal.com.au/wp-conte ... urgery.pdf
41M Australia
2018 Dx RC
G2 EMVI LVI, 4 liver mets
pT3N1aM1a Stage IVa MSS NRAS G13R
CEA 14>2>32>16>19>30>140>70
11/18 FOLFOX
3/19 Liver resection
5/19 Pelvic IMRT
7/19 ULAR
8/19 Liver met
8/19 FOLFOX, FOLFOXIRI, FOLFIRI
12/19 Liver resection
NED 2 years
11/21 Liver met, PALN, lung nodules
3/22 PVE, lymphadenectomy, liver SBRT
10/22 PALN SBRT
11/22 Liver mets, peri nodule. Xeloda+Bev
4/23 XELIRI+Bev
9/23 ATRIUM trial
12/23 Modified FOLFIRI+Bev
3/24 VAXINIA (CF33 + hNIS) trial
2018 Dx RC
G2 EMVI LVI, 4 liver mets
pT3N1aM1a Stage IVa MSS NRAS G13R
CEA 14>2>32>16>19>30>140>70
11/18 FOLFOX
3/19 Liver resection
5/19 Pelvic IMRT
7/19 ULAR
8/19 Liver met
8/19 FOLFOX, FOLFOXIRI, FOLFIRI
12/19 Liver resection
NED 2 years
11/21 Liver met, PALN, lung nodules
3/22 PVE, lymphadenectomy, liver SBRT
10/22 PALN SBRT
11/22 Liver mets, peri nodule. Xeloda+Bev
4/23 XELIRI+Bev
9/23 ATRIUM trial
12/23 Modified FOLFIRI+Bev
3/24 VAXINIA (CF33 + hNIS) trial
Return to “Colon Talk - Colon cancer (colorectal cancer) support forum”
Who is online
Users browsing this forum: Google [Bot], Olivia77 and 264 guests