Hello,
My dad recently had open heart surgery because of two clogged arteries. After couple of months he was having some bleeding in his bowels. Apparently he thought it was usual after surgery. After about a week or so he almost collapsed and got admitted in to hospital. After blood examination he was having only half the amount of blood by volume. He got blood infusion and was ok. After about three months he lost the blood again and after endoscopy, colonoscopy they found a tumor. They did CTC scan yesterday but radiologist was too busy to explain the results back to us.
Below is the report from Radiologist. We are not sure what it is and if it is cancer what stage it is and how serious it is.
The question I have is is the surgery first line of defense at this moment? Or could we treat by using chemo/radiation? If surgery is a must, do my dad need to undergo chemo and or radiation? We are still waiting on the biopsy report and then we could consult an oncologist. I was doing some online reading and fortunately stumbled upon this forum. I read some posts and it did give me some idea.
I understand the advice I get may be from non-professionals. I will be consulting an Oncologist but it is going to be at least next Monday. I would like to see what the below passages mean in the mean time. Thanks for your time.
Report from Radiologist
Colo-colic intusucception of ascending colon noted with a large ill defined polypoidal soft tissue density, moderately enhancing mass measuring approximately 7x4.4 cm epicentered in ascending colon as its lead point, not causing any significant obstructin/dilatation of bowel loops proximal to it.
Cirucumferential nodular wall thiceking with submucosal oedema noted extending into hepatic flexure and proximal half of treansverse colon. Multiple draining mildly enhancing mesenteric lymphnodes noted in righ half of abdomen, largest measuring 1.5x0.9 cm in right iliac fossa and 1.1 x 1cm in central mesentry. Prominent vasa rectal seen supplying ascending colon. Mild perienteric fat stranding noted.
Base of caecum, ileo-caecal junction and appendix appear grossly normal.
Visualized sections of both lung bases, reveal multiple subsegmental atelectatic bands with bilateral mild defree pleural effusion. Peribronchovascular ground glass haze noted in both lungs (rught>left) indicating active insult. No evidence of any obvious focal lesions.
Bone window reveals no obvious eveidence of any focal bone lesions. Age related spondylotic changes in underlying spine.
Impression
Colo-colic intusucception of ascending colon noted with a large ill defined polypoidal soft tissue density, moderately enhancing mass epicentered in ascending colon as its lead point, not causing any significant obstruction/dilatation of bowel loops proximal to it. Circumferential nodular wall thickening with submucosal oedema extending into hepatic flexure and proximal half of transverse colon with multiple draining mildly enhancing mesenteric lymphnodes and prominent vasa rectae seen supplying ascending colon associated with mild perienteric fat stranding noted - Likely of malignant etiology with local metastases to mesentric lymph nodes.
My dad just got diagnosed with colon cancer
Re: My dad just got diagnosed with colon cancer
I am sorry to hear about your father...he is lucky to have your support. I am assuming that he had a biopsy at the time of his colonoscopy? The next step would definitely be consultation with an oncologist, and probably a colorectal surgeon as well. Neoadjuvant chemoradiation (or chemotherapy) is the standard of care for rectal cancer, but with colon cancer, it would be more typical to have surgical resection first (for stage 3 or lower). But everyone is different, and it is becoming more common for people to have chemo first, even for stage 3 disease.
I do definitely recommend that he see an oncologist at a major cancer center if at all possible; don't be afraid to ask for a second opinion! And knowing as many details about the cancer is vital in order for him to get the most appropriate treatment (at the very least MSS vs MSI). I wish him luck...the first few weeks are so stressful and overwhelming, but it does get easier once you have a treatment plan in place!
I do definitely recommend that he see an oncologist at a major cancer center if at all possible; don't be afraid to ask for a second opinion! And knowing as many details about the cancer is vital in order for him to get the most appropriate treatment (at the very least MSS vs MSI). I wish him luck...the first few weeks are so stressful and overwhelming, but it does get easier once you have a treatment plan in place!
Dx 12/2014 T3N2MX (distant LPLN) low rectal
12/2014-4/2015: FOLFOX (8 cycles)
4/2015-6/2015: 28 cycles of chemoradiation with xeloda, SBRT
8/2015: Robotic APR with iliac node dissection; path showed ypT0,ypN0 (complete pathological response).
11/2015 scans clear, CEA 2.1
11/2015 parastomal hernia repair
3/2016 CEA 1.7, scans stable...
6/2020 5 years of normal CEA and stable scans
Now dealing with pyoderma gangrenosum.
Totally disabled due to oxaliplatin induced neuropathy and dysautonomia
12/2014-4/2015: FOLFOX (8 cycles)
4/2015-6/2015: 28 cycles of chemoradiation with xeloda, SBRT
8/2015: Robotic APR with iliac node dissection; path showed ypT0,ypN0 (complete pathological response).
11/2015 scans clear, CEA 2.1
11/2015 parastomal hernia repair
3/2016 CEA 1.7, scans stable...
6/2020 5 years of normal CEA and stable scans
Now dealing with pyoderma gangrenosum.
Totally disabled due to oxaliplatin induced neuropathy and dysautonomia
Re: My dad just got diagnosed with colon cancer
Thanks Hawkowl for the response.
Yes he had biopsy at the time of Colonoscopy. The doctor said it will take about 4 days for the results. They said it may be a tumor and need surgery to remove it and he was pretty persistent. But my concern was he is Endocrinologist and not an Oncologist. So I was surprised why he was pressing us to have a surgery without an expert opinion ie, an Oncologist.
How do you rate Moffitt Cancer Center? I live very close to this place.
Yes he had biopsy at the time of Colonoscopy. The doctor said it will take about 4 days for the results. They said it may be a tumor and need surgery to remove it and he was pretty persistent. But my concern was he is Endocrinologist and not an Oncologist. So I was surprised why he was pressing us to have a surgery without an expert opinion ie, an Oncologist.
How do you rate Moffitt Cancer Center? I live very close to this place.
Re: My dad just got diagnosed with colon cancer
Moffitt is very well respected. My sister is an internist in the Tampa Bay area and I seriously considered undergoing treatment there, but in the end opted to stay closer to home (Minnesota at that time)
Dx 12/2014 T3N2MX (distant LPLN) low rectal
12/2014-4/2015: FOLFOX (8 cycles)
4/2015-6/2015: 28 cycles of chemoradiation with xeloda, SBRT
8/2015: Robotic APR with iliac node dissection; path showed ypT0,ypN0 (complete pathological response).
11/2015 scans clear, CEA 2.1
11/2015 parastomal hernia repair
3/2016 CEA 1.7, scans stable...
6/2020 5 years of normal CEA and stable scans
Now dealing with pyoderma gangrenosum.
Totally disabled due to oxaliplatin induced neuropathy and dysautonomia
12/2014-4/2015: FOLFOX (8 cycles)
4/2015-6/2015: 28 cycles of chemoradiation with xeloda, SBRT
8/2015: Robotic APR with iliac node dissection; path showed ypT0,ypN0 (complete pathological response).
11/2015 scans clear, CEA 2.1
11/2015 parastomal hernia repair
3/2016 CEA 1.7, scans stable...
6/2020 5 years of normal CEA and stable scans
Now dealing with pyoderma gangrenosum.
Totally disabled due to oxaliplatin induced neuropathy and dysautonomia
-
DarknessEmbraced
- Posts: 3817
- Joined: Sat Nov 01, 2014 4:54 pm
- Facebook Username: Riann Fletcher
- Location: New Brunswick, Canada
Re: My dad just got diagnosed with colon cancer
I'm sorry you and your father are going through this and hope you won't have to wait long for the pathology report.*hugs*
Diagnosed 10/28/14, age 36
Colon Resection 11/20/14, LAR (no illeo)
Stage 2a colon cancer, T3NOMO
Lymph-vascular invasion undetermined
0/22 lymph nodes
No chemo, no radiation
Clear Colonoscopy 04/29/15
NED 10/20/15
Ischemic Colitis 01/21/16
NED 11/10/16
CT Scan moved up due to high CEA 08/21/17
NED 09/25/17
NED 12/21/18
Clear colonoscopy 09/23/19
Clear 5 year scans 11/21/19- Considered cured!
Colon Resection 11/20/14, LAR (no illeo)
Stage 2a colon cancer, T3NOMO
Lymph-vascular invasion undetermined
0/22 lymph nodes
No chemo, no radiation
Clear Colonoscopy 04/29/15
NED 10/20/15
Ischemic Colitis 01/21/16
NED 11/10/16
CT Scan moved up due to high CEA 08/21/17
NED 09/25/17
NED 12/21/18
Clear colonoscopy 09/23/19
Clear 5 year scans 11/21/19- Considered cured!
Re: My dad just got diagnosed with colon cancer
the_dude wrote:Thanks Hawkowl for the response.
Yes he had biopsy at the time of Colonoscopy. The doctor said it will take about 4 days for the results. They said it may be a tumor and need surgery to remove it and he was pretty persistent. But my concern was he is Endocrinologist and not an Oncologist. So I was surprised why he was pressing us to have a surgery without an expert opinion ie, an Oncologist.
How do you rate Moffitt Cancer Center? I live very close to this place.
My point guy was a GI specialist and his staff did most of the work connecting me with oncologists and radiation doctors, both local and remote for second opinions. Someone has to play point until you get transferred to an oncologist. I suppose a PCP could do this as well. In my case, control for treatment passed to the local oncologist until after Chemo and Radiation were done and then it was transferred to the Surgeon. It goes back to the Oncologist for me in a week.
US News and World Report rate Moffitt as sixth best in the country for cancer. So I'd be fine with them personally.
This will be a tough road for your dad and your family but there are lots of people that get through it and you have a big community here to help you and your dad along the way. The vast majority of folks on the board have cancer, had it or have/had a relative with it.
6/17: ER rectal bleeding; Colonoscopy
7/17: 3B rectal. T3N1bM0. 5.2 4.5 4.3 cm. Lymphs: 6 x 4 mm, 8 x 6, 5 x 5
7/17-9/17: Xeloda radiation
7/5: CEA 2.7; 8/16: 1.9; 11/30: 0.6; 12/20 1.4; 1/10 1.8; 1/31 2.2; 2/28 2.6; 4/10 2.8; 5/1 2.8; 5/29 3.2; 7/13 4.5; 8/9 2.8, 2/12 1.2
MSS, KRAS G12D
10/17: 2.7 2.2 1.6 cm (-90%). Lymphs: 3 x 3 mm (-62.5%), 4 x 3 (-75%), 5 x 3 (-40%). 5.1 CM from AV
10/17: LAR, Temp Ileostomy, Path Complete Response
CapeOx (8) 12/17-6/18
7/18: Reversal, Port Removal
2/19: Clean CT
7/17: 3B rectal. T3N1bM0. 5.2 4.5 4.3 cm. Lymphs: 6 x 4 mm, 8 x 6, 5 x 5
7/17-9/17: Xeloda radiation
7/5: CEA 2.7; 8/16: 1.9; 11/30: 0.6; 12/20 1.4; 1/10 1.8; 1/31 2.2; 2/28 2.6; 4/10 2.8; 5/1 2.8; 5/29 3.2; 7/13 4.5; 8/9 2.8, 2/12 1.2
MSS, KRAS G12D
10/17: 2.7 2.2 1.6 cm (-90%). Lymphs: 3 x 3 mm (-62.5%), 4 x 3 (-75%), 5 x 3 (-40%). 5.1 CM from AV
10/17: LAR, Temp Ileostomy, Path Complete Response
CapeOx (8) 12/17-6/18
7/18: Reversal, Port Removal
2/19: Clean CT
Re: My dad just got diagnosed with colon cancer
Hi,
I am sorry to hear about your father. This is a a great support group. I was alone in the recovery room when my mom's GI told me that she had rectal cancer, and when he told me, it was like a blur! Then, he told me that it didn't look that good and she will most likely have a bag for the rest of her life. I was so confused, angry, upset, emotional. I was mad that he was so RAW and honest.. like I felt violated! My mom was still out from her cocktail drug they gave her when going in. I was angry to be the only one finding out. I was mad that my dad wasn't there with me. I was indenial if that makes sense. You are going to be going through so many emotions, ups and down's. Then, he referred us to this surgeon which had the worst reviews on Yelp.com. There was no way that I would send my mom to that surgeon. Just try to be there for him as much as possible. Prior to my mom's DX, my dad had triple bi pass surgery and he had a complication, he made it but it was all such a crazy year for our family. After my mom's DX, I had to switch her insurance around to get her to the best specialist, surgeon, oncologist and hospitals. It was a whirlwind but we made it work! My mom had surgery on Oct 17 and she had a very difficult recovery, but she came through. The got most of the cancer out and no lymph's were involved. She had a "Near Path Response" and has to do the clean up chemo in a couple of weeks. Good news is that they got all the cancer and there were a few cancer cells left. She still is very homebound and is very embarrassed about her pouch. I always tell her, sometimes people lose something to gain something. I do feel that I was a big part of saving my mom's life. She is a hard head. She lives on the same street as me just two homes down so we see each other la a lot. I had to push her to get a colonoscopy and thankfully she went. I studied medical allied health and now studying to become an RN. I was kinda upset at her general dr. cause he kept saying that she made have Lupus, bone cancer, than it was Osteoporosis. My mom didn't have a colonoscopy done in almost 9 years.. and even though he recommended it three years prior, he could of recommended her again. Sometimes, Dr. don't know it all! I wish you the best and try not to google every little thing cause it will drive you up the wall. I had to stop. Have a good night!
I am sorry to hear about your father. This is a a great support group. I was alone in the recovery room when my mom's GI told me that she had rectal cancer, and when he told me, it was like a blur! Then, he told me that it didn't look that good and she will most likely have a bag for the rest of her life. I was so confused, angry, upset, emotional. I was mad that he was so RAW and honest.. like I felt violated! My mom was still out from her cocktail drug they gave her when going in. I was angry to be the only one finding out. I was mad that my dad wasn't there with me. I was indenial if that makes sense. You are going to be going through so many emotions, ups and down's. Then, he referred us to this surgeon which had the worst reviews on Yelp.com. There was no way that I would send my mom to that surgeon. Just try to be there for him as much as possible. Prior to my mom's DX, my dad had triple bi pass surgery and he had a complication, he made it but it was all such a crazy year for our family. After my mom's DX, I had to switch her insurance around to get her to the best specialist, surgeon, oncologist and hospitals. It was a whirlwind but we made it work! My mom had surgery on Oct 17 and she had a very difficult recovery, but she came through. The got most of the cancer out and no lymph's were involved. She had a "Near Path Response" and has to do the clean up chemo in a couple of weeks. Good news is that they got all the cancer and there were a few cancer cells left. She still is very homebound and is very embarrassed about her pouch. I always tell her, sometimes people lose something to gain something. I do feel that I was a big part of saving my mom's life. She is a hard head. She lives on the same street as me just two homes down so we see each other la a lot. I had to push her to get a colonoscopy and thankfully she went. I studied medical allied health and now studying to become an RN. I was kinda upset at her general dr. cause he kept saying that she made have Lupus, bone cancer, than it was Osteoporosis. My mom didn't have a colonoscopy done in almost 9 years.. and even though he recommended it three years prior, he could of recommended her again. Sometimes, Dr. don't know it all! I wish you the best and try not to google every little thing cause it will drive you up the wall. I had to stop. Have a good night!
Caregiver/daughter to dear mother age 78, dx 5/09/17 because of me!! 
Rectal CA Stage 3 low-grade adenocarcinoma- 6 cm
Neoadjuvant start 7/10/17 ended 08/16/17
3D Lap. surgery @ Keck USC, Dr. Sang Lee 10/17/17 temp ileostomy
11/1 hospitalized abscess/hernia - home 11/06/17 antibiotics
NO LYMPHS INVOLVED! NEAR PATHOLOGICAL RESPONSE! YAY!
Took her last chemo med 05/10/18! Ileo reversal 07/24/18
1st BM after reversal 07/25/18 Anal Fissure 8/15/18
Me:1st Colonoscopy age 38. 08/17 Benign polp.
Rectal CA Stage 3 low-grade adenocarcinoma- 6 cm
Neoadjuvant start 7/10/17 ended 08/16/17
3D Lap. surgery @ Keck USC, Dr. Sang Lee 10/17/17 temp ileostomy
11/1 hospitalized abscess/hernia - home 11/06/17 antibiotics
NO LYMPHS INVOLVED! NEAR PATHOLOGICAL RESPONSE! YAY!
Took her last chemo med 05/10/18! Ileo reversal 07/24/18
1st BM after reversal 07/25/18 Anal Fissure 8/15/18
Me:1st Colonoscopy age 38. 08/17 Benign polp.
Re: My dad just got diagnosed with colon cancer
Hi,
I am sorry to hear about your father. This is a a great support group. I was alone in the recovery room when my mom's GI told me that she had rectal cancer, and when he told me, it was like a blur! Then, he told me that it didn't look that good and she will most likely have a bag for the rest of her life. I was so confused, angry, upset, emotional. I was mad that he was so RAW and honest.. like I felt violated! My mom was still out from her cocktail drug they gave her when going in. I was angry to be the only one finding out. I was mad that my dad wasn't there with me. I was indenial if that makes sense. You are going to be going through so many emotions, ups and down's. Then, he referred us to this surgeon which had the worst reviews on Yelp.com. There was no way that I would send my mom to that surgeon. Just try to be there for him as much as possible. Prior to my mom's DX, my dad had triple bi pass surgery and he had a complication, he made it but it was all such a crazy year for our family. After my mom's DX, I had to switch her insurance around to get her to the best specialist, surgeon, oncologist and hospitals. It was a whirlwind but we made it work! My mom had surgery on Oct 17 and she had a very difficult recovery, but she came through. The got most of the cancer out and no lymph's were involved. She had a "Near Path Response" and has to do the clean up chemo in a couple of weeks. Good news is that they got all the cancer and there were a few cancer cells left. She still is very homebound and is very embarrassed about her pouch. I always tell her, sometimes people lose something to gain something. I do feel that I was a big part of saving my mom's life. She is a hard head. She lives on the same street as me just two homes down so we see each other la a lot. I had to push her to get a colonoscopy and thankfully she went. I studied medical allied health and now studying to become an RN. I was kinda upset at her general dr. cause he kept saying that she made have Lupus, bone cancer, than it was Osteoporosis. My mom didn't have a colonoscopy done in almost 9 years.. and even though he recommended it three years prior, he could of recommended her again. Sometimes, Dr. don't know it all! I wish you the best and try not to google every little thing cause it will drive you up the wall. I had to stop. Have a good night!
I am sorry to hear about your father. This is a a great support group. I was alone in the recovery room when my mom's GI told me that she had rectal cancer, and when he told me, it was like a blur! Then, he told me that it didn't look that good and she will most likely have a bag for the rest of her life. I was so confused, angry, upset, emotional. I was mad that he was so RAW and honest.. like I felt violated! My mom was still out from her cocktail drug they gave her when going in. I was angry to be the only one finding out. I was mad that my dad wasn't there with me. I was indenial if that makes sense. You are going to be going through so many emotions, ups and down's. Then, he referred us to this surgeon which had the worst reviews on Yelp.com. There was no way that I would send my mom to that surgeon. Just try to be there for him as much as possible. Prior to my mom's DX, my dad had triple bi pass surgery and he had a complication, he made it but it was all such a crazy year for our family. After my mom's DX, I had to switch her insurance around to get her to the best specialist, surgeon, oncologist and hospitals. It was a whirlwind but we made it work! My mom had surgery on Oct 17 and she had a very difficult recovery, but she came through. The got most of the cancer out and no lymph's were involved. She had a "Near Path Response" and has to do the clean up chemo in a couple of weeks. Good news is that they got all the cancer and there were a few cancer cells left. She still is very homebound and is very embarrassed about her pouch. I always tell her, sometimes people lose something to gain something. I do feel that I was a big part of saving my mom's life. She is a hard head. She lives on the same street as me just two homes down so we see each other la a lot. I had to push her to get a colonoscopy and thankfully she went. I studied medical allied health and now studying to become an RN. I was kinda upset at her general dr. cause he kept saying that she made have Lupus, bone cancer, than it was Osteoporosis. My mom didn't have a colonoscopy done in almost 9 years.. and even though he recommended it three years prior, he could of recommended her again. Sometimes, Dr. don't know it all! I wish you the best and try not to google every little thing cause it will drive you up the wall. I had to stop. Have a good night!
Caregiver/daughter to dear mother age 78, dx 5/09/17 because of me!!
Rectal CA Stage 3 low-grade adenocarcinoma- 6 cm
Neoadjuvant start 7/10/17 ended 08/16/17
3D Lap. surgery @ Keck USC, Dr. Sang Lee 10/17/17 temp ileostomy
11/1 hospitalized abscess/hernia - home 11/06/17 antibiotics
NO LYMPHS INVOLVED! NEAR PATHOLOGICAL RESPONSE! YAY!
Took her last chemo med 05/10/18! Ileo reversal 07/24/18
1st BM after reversal 07/25/18 Anal Fissure 8/15/18
Me:1st Colonoscopy age 38. 08/17 Benign polp.
Rectal CA Stage 3 low-grade adenocarcinoma- 6 cm
Neoadjuvant start 7/10/17 ended 08/16/17
3D Lap. surgery @ Keck USC, Dr. Sang Lee 10/17/17 temp ileostomy
11/1 hospitalized abscess/hernia - home 11/06/17 antibiotics
NO LYMPHS INVOLVED! NEAR PATHOLOGICAL RESPONSE! YAY!
Took her last chemo med 05/10/18! Ileo reversal 07/24/18
1st BM after reversal 07/25/18 Anal Fissure 8/15/18
Me:1st Colonoscopy age 38. 08/17 Benign polp.
-
O Stoma Mia

- Posts: 1709
- Joined: Sat Jun 22, 2013 6:29 am
- Location: On vacation. Off-line for now.
Re: My dad just got diagnosed with colon cancer
the_dude wrote: ...I would like to see what the below passages mean in the mean time. Thanks for your time.
Report from Radiologist
Colo-colic intusucception of ascending colon noted with a large ill defined polypoidal soft tissue density, moderately enhancing mass measuring approximately 7x4.4 cm epicentered in ascending colon as its lead point, not causing any significant obstructin/dilatation of bowel loops proximal to it.
Cirucumferential nodular wall thiceking with submucosal oedema noted extending into hepatic flexure and proximal half of treansverse colon. Multiple draining mildly enhancing mesenteric lymphnodes noted in righ half of abdomen, largest measuring 1.5x0.9 cm in right iliac fossa and 1.1 x 1cm in central mesentry. Prominent vasa rectal seen supplying ascending colon. Mild perienteric fat stranding noted.
Base of caecum, ileo-caecal junction and appendix appear grossly normal.
Visualized sections of both lung bases, reveal multiple subsegmental atelectatic bands with bilateral mild defree pleural effusion. Peribronchovascular ground glass haze noted in both lungs (rught>left) indicating active insult. No evidence of any obvious focal lesions.
Bone window reveals no obvious eveidence of any focal bone lesions. Age related spondylotic changes in underlying spine.
Impression
Colo-colic intusucception of ascending colon noted with a large ill defined polypoidal soft tissue density, moderately enhancing mass epicentered in ascending colon as its lead point, not causing any significant obstruction/dilatation of #bowel loops proximal to it. Circumferential nodular wall thickening with submucosal oedema extending into hepatic flexure and proximal half of transverse colon with multiple draining mildly enhancing mesenteric lymphnodes and prominent vasa rectae seen supplying ascending colon associated with mild perienteric fat stranding noted - Likely of malignant etiology with local metastases to mesentric lymph nodes.
I will give my own opinion, but I am not a scientist or medical professional.
The Radiologist Report comes in two parts. The top part contains the "facts" that the scan reveals. The bottom part contains the personal opinion of the Radiologist after his/her review of the basic facts. The most relevant part is the very last sentence, where the Radiologist gives his/her overall impression.
From the final sentence, it appears that the Radiologist thinks that this is likely a Stage III diagnosis, such as T4b N1b M0. This is just my layman's opinion.
I would say T4b because of the term "intussusception" used in the description,. which seems to imply that the tumor has grown outside the colon wall and immediately back into another adjacent loop in the colon.
I would say N1b because it seems that at least 2 or 3 of the local lymph nodes are possibly involved with metastases.
I would say M0 because all of the problems in the liver and lungs seem to be benign. In particular, the problems in the lungs sre likely due to injuries sustained during the previous open heart surgery and not to cancer.
Thus, in the TNM staging system this would equate to Stage IIIC (Group 3) which is shown here:
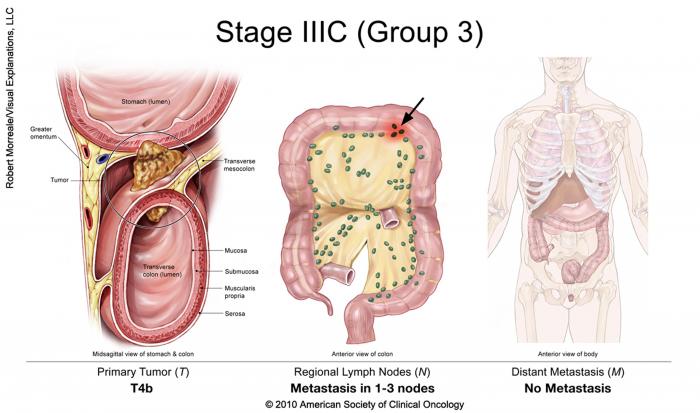
Your father is very lucky to have you as an advocate and information gatherer. If the diagnosis is in fact a Stage III diagnosis, then the recommended standard of care would probably be surgery to remove the tumor and local lymph nodes, followed by a 6-month regimen of "mop-up" chemotherapy to take care of any circulating cancer cells that might be left over after surgery. The surgery would have to be done by a Board Certified colorectal surgeon.
Radiation is not normally done for tumors in the ascending colon.
EDIT
There are 2 Board Certified colorectal surgeons affiliated with Moffitt Cancer Center. For the hospital as a whole, here is their US News & World Report scorecard on Colon Cancer Surgery:
https://health.usnews.com/best-hospitals/area/fl/moffitt-cancer-center-6391069/colon-cancer-surgery
.
.
Return to “Colon Talk - Colon cancer (colorectal cancer) support forum”
Who is online
Users browsing this forum: No registered users and 70 guests