O Stoma Mia wrote:lakeswim wrote:... Would you say radiation side effects are much worse than chemo - or does that highly depend? And must I even DO radiation? ...
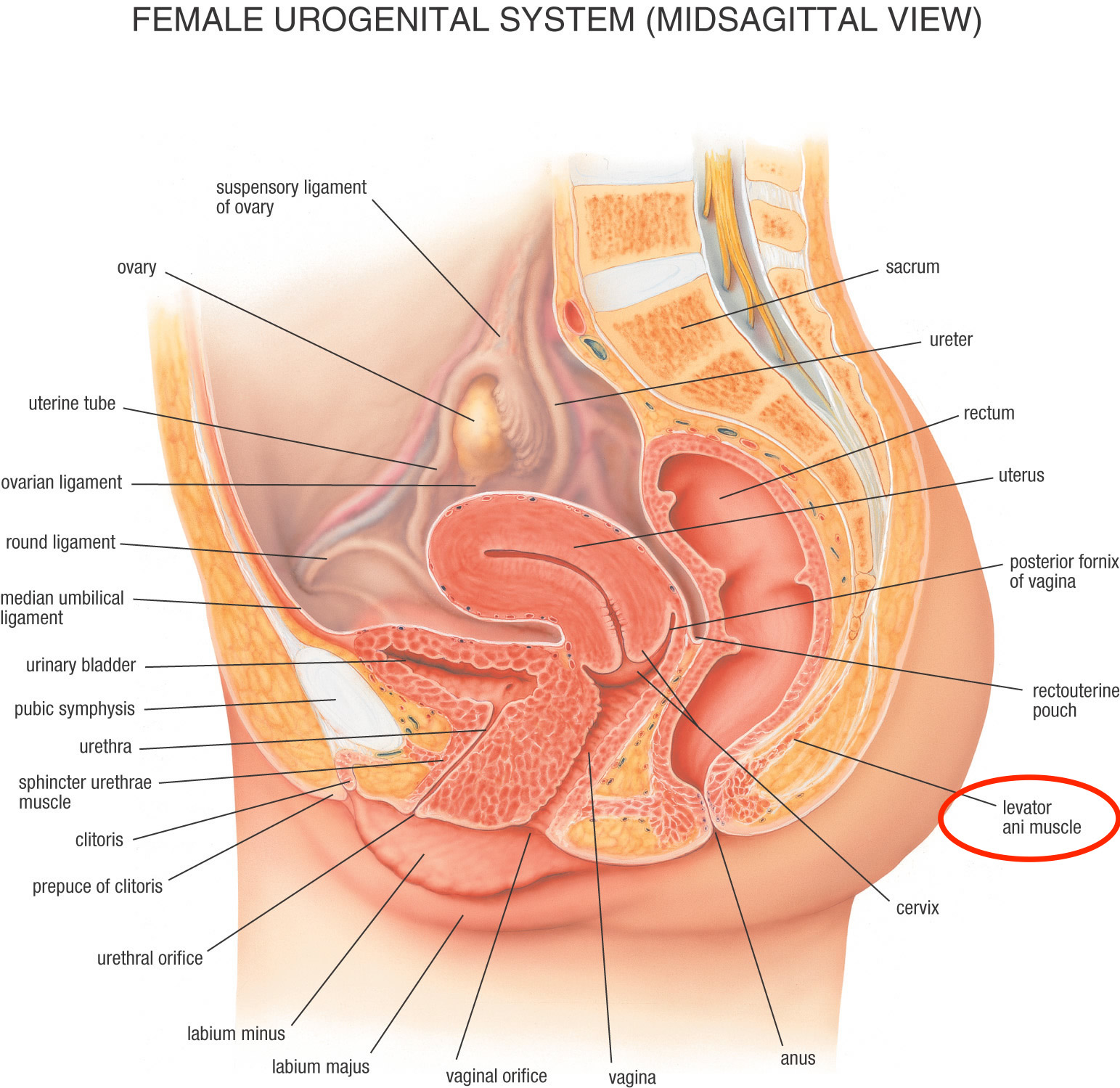
I don't really know, but I think it probably depends. I noticed on the clinical trial's protocol that they will be using IMRT (Intensity Modulated Radiation Therapy) for the radiation phase. This procedure allows the radiation oncologist to target which parts of which organs receive the full intensity radiation, and which organs receive minimal radiation. Since your tumor is on the anterior wall of the rectum at the second haustral fold, this suggests that your radiation will be focused mainly in that area, which is very close to the uterus and not too far away from the upper part of the vagina (see diagram below). This may mean that there might be some collateral radiation damage to the female uro-genital area.
Diagram:
http://www.stepwards.com/wp-content/uploads/2016/06/Urogenital-system-female-anatomy-photographs-sacrum-ureter-rectum-uterus-posterior-fornix-vagina-rectouterine-pouch-levator-ani-muscle-cervix-anus-cl.jpg
Here is some information on IMRT and radiation:
Targeted rectal radiation: IMRT / IGRT
http://coloncancersupport.colonclub.com/viewtopic.php?f=1&t=48936&p=372445#p372445
GOOD STUFF! Thank you! As usual, you have great info and I can't wait to return from Cleveland and review it all and follow up with questions. I BELIEVE that I will get targeted radiation regardless of whether or not I am on the trial. (They kept saying it would be "same treatment" - just flipped.) But a good question to ask both in my appt tomorrow and in f/u discussions on the trial with my team here.
I assume when I return, I will ALSO have more questions about deciding on second opinions - and traveling for parts of treatment. I will have to search for links on that but if you have any advice, I appreciate it.
Thank you - as always - for your help and support.

{kind=link}