Page 1 of 2
LAR Syndrome and laparoscopic surgery, new paper on origins
Posted: Thu Nov 16, 2017 12:32 am
by chrisca
I just had a visit with my GI doc. A new paper is out on LAR syndrome. While it doesn't provide any treatment breakthroughs, it gives encouraging news that researchers are homing in on the cause. It's at:
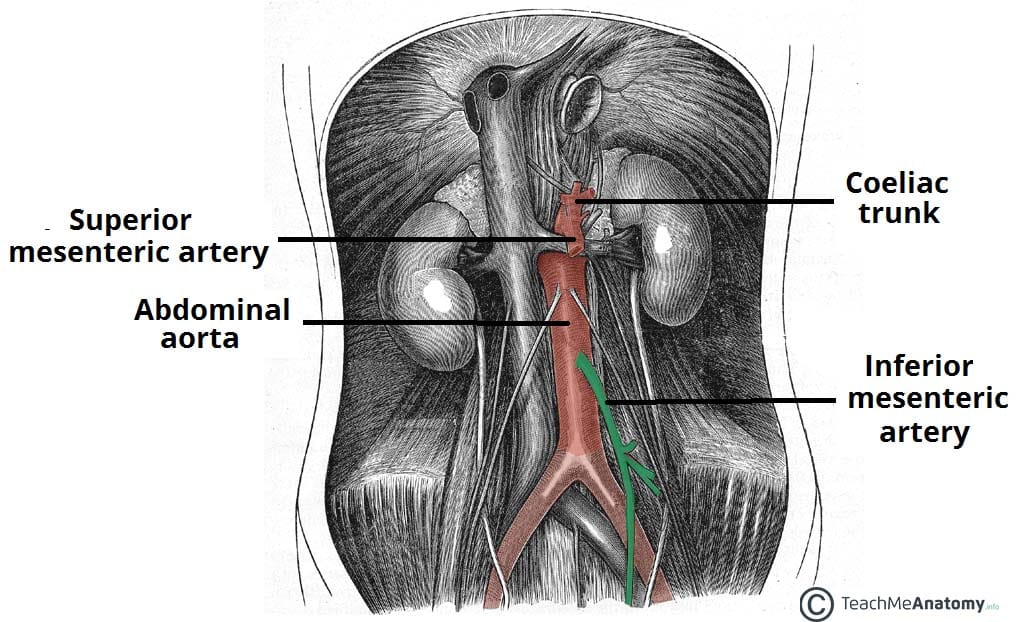
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4991969/. A major cause appears to be loss of nerve connections along the inferior mesenteric artery (IMA). An interesting excerpt from the paper:
It is very likely that much of what is recognized as LAR syndrome is actually related to what happens to the autonomic innervation of the neorectum during the course of the extensive mobilization that occurs during a LAR. The authors have observed in the operating room that after the complete mobilization and division of bowel required as part of a LAR (in preparation for a coloanal anastomosis), there are very strong contractions that randomly take place in the distal transverse and descending colon: they never start or progress into the mid- or proximal transverse colon. We have hypothesized that the disordered bowel function, known as LAR syndrome, is a result of motility changes seen in the left colon following extrinsic denervation that occurs with the extensive mobilization performed during these operations.
My GI doc mentioned that with the increasing popularity of laparoscopic procedures for rectal resection, very high ligation of the IMA is usually done. This is the worst possible scenario for LAR syndrome risk.
Anyone contemplating laparoscopic rectal resection should be aware of this risk and ask the surgeon about how the IMA ligation will be done. While laparoscopic surgery has a quicker recovery, it could leave one with lifelong consequences that might not happen if it's possible to choose open surgery and low ligation of the IMA. Whether that is possible or not depends on a number of factors, and can only be determined for certain during the procedure. But be informed, and discuss the risks with your doctor beforehand.
Re: LAR Syndrome and laparoscopic surgery, new paper on origins
Posted: Thu Nov 16, 2017 1:06 am
by O Stoma Mia
Thanks for posting this. This article has new and very important information for all patients who are scheduled for rectal or recto-sigmoid resections.
This is basically an issue with Informed Consent. I think that laparoscopic surgeons know quite well what the risks are, but they are not so quick to convey this information to the patient during the Informed Consent procedure. Thus, I think it is up to the patient to bring up issues like this in the question-and-answer phase of the Informed Consent Form signing.
Here is a typical Informed Consent form for Laparoscopic Surgery but, as you can see, it doesn’t explictly mention anything about risks associated when the procedure is performed in the LAR context.
https://www.health.qld.gov.au/consent/documents/shared_file_46.pdfSo, what I would suggest is that if patients have just been diagnosed with rectal or recto-sigmoid cancer and have not yet had surgery, then they should first educate themselves about the anatomical requirements for successful sphincter-sparing surgery and successful total mesorectal excision (TME) surgery.
Medical school textbooks are very specific about what should and should not be done to insure good long-term outcomes for bowel control. The textbooks even have
pictures showing which structures (blood vessels, nerve bundles, etc.) need to be preserved in order to have a successful surgery. Patients who are being scheduled for rectal surgery should insure that they select a highly qualified, experienced Board Certified colorectal surgeon for the surgery, especially if it is going to be a laparoscopic surgery, since laparoscopic surgeries are more difficult for surgeons to handle correctly, given all of the constraints involved.
Re: LAR Syndrome and laparoscopic surgery, new paper on origins
Posted: Thu Nov 16, 2017 10:08 am
by NHMike
I didn't know about these risks but I didn't have a choice in the surgical approach. The surgeon decided on open surgery though I had assumed laparoscopic. Then I saw that it was laparoscopic-assisted shortly before the surgery and there's where I figured that I'd have an open procedure. Which is what happened. So yes, recovery is taking longer and I've got that huge honking scar now. But it sounds like we avoided risk of this other potential problem.
Re: LAR Syndrome and laparoscopic surgery, new paper on origins
Posted: Thu Nov 16, 2017 11:42 am
by heiders33
I was not aware of these risks associated with laparoscopic surgery either. It was considered a victory when my surgery was done entirely laparoscopically, since there was a chance it wouldn't be. But this makes me not so sure. However, I have a very experienced, board-certified colorectal surgeon. I see him tomorrow and will ask him these questions. Thanks for posting this!
Re: LAR Syndrome and laparoscopic surgery, new paper on origins
Posted: Thu Nov 16, 2017 12:57 pm
by NHMike
heiders33 wrote:I was not aware of these risks associated with laparoscopic surgery either. It was considered a victory when my surgery was done entirely laparoscopically, since there was a chance it wouldn't be. But this makes me not so sure. However, I have a very experienced, board-certified colorectal surgeon. I see him tomorrow and will ask him these questions. Thanks for posting this!
I think that a Board-Certified CRC Surgeon would make the best choice for the individual patient.
I asked my surgeon why she didn't do laparoscopic only and she said that my pelvis was quite small. She's trained in Robotic as well and that wasn't used. I assume that she had very good reasons why she chose the approach that she did. Yes, the recovery will be longer but I will recover.
Re: LAR Syndrome and laparoscopic surgery, new paper on origins
Posted: Thu Nov 16, 2017 4:03 pm
by susie0915
I remember the surgeon told me during my consultation, that women are generally easier to operate on as they tend to have a wider pelvis. I ended up having open surgery 5 weeks later to take care of my blockage, and yes the recovery was tougher, but it was okay. So I have both laparoscopic scars and a vertical incision from above the belly button down to the pubic bone. I did get an infection in the incision that I had to pack with gauze a couple times a day, but it was not that bad. You sound like you are healing and recovering pretty well.
Re: LAR Syndrome and laparoscopic surgery, new paper on origins
Posted: Thu Nov 16, 2017 4:43 pm
by NHMike
susie0915 wrote:I remember the surgeon told me during my consultation, that women are generally easier to operate on as they tend to have a wider pelvis. I ended up having open surgery 5 weeks later to take care of my blockage, and yes the recovery was tougher, but it was okay. So I have both laparoscopic scars and a vertical incision from above the belly button down to the pubic bone. I did get an infection in the incision that I had to pack with gauze a couple times a day, but it was not that bad. You sound like you are healing and recovering pretty well.
I grew up in pretty rough financial conditions and we often skipped meals so I was pretty skinny growing up which probably accounts for the narrow pelvis. It sounds like you had colon surgery which accounts for the differences in our cuts. Mine is horizontal, about five inches below the belly button and about five inches long. So I have to be very careful about any folding motions that stress that direction. I would think that a vertical cut would be more difficult for recovery because you have the folding issue as well as dealing with sideways stresses.
They put in one staple on the left, one in the belly button, one on the upper right and a drain in the lower right. The drain hole is already covered over with skin. There's still a bandage on top of the right one but that's because it's so close to the Ileostomy. There are no bandages on the left side anymore. Things are going well. Some minor aches here and there and I do tend to overdo things so some of those aches are my fault. But nothing bad enough to take pain medication of any kind. So far.
Re: LAR Syndrome and laparoscopic surgery, new paper on origins
Posted: Thu Nov 16, 2017 7:07 pm
by Big Jay
Interesting paper. I was especially interested in the research into the length of the remaining rectal stump and the method of reconnection. Basically the more rectum the better with a minimum of 4cm for best results. Also some sort of reservoir, be it J-Pouch, or Side-End, is significantly better in both the short and long term than a straight connection.
I met w/ the surgeon last week it sounds like his plan is guaranteed to result in LARS.
My tumor has completely disappeared after radiation but, when it existed, it was at 9cm from the anal verge. Still the surgeon wants to cut out my entire rectum down to the dentate line. I pointed out that he probably could safely leave 4-5cm of rectum but he told me that it's hard to make that measurement during surgery. So it's easier for him cut everything out. When I objected he said "you won't miss those extra centimeters". According to this research I will certainly miss them.
He also insists that a straight connection is just the same as a pouch. Again, per this research, that isn't the case. Guess it's time to find a different surgeon.
Re: LAR Syndrome and laparoscopic surgery, new paper on origins
Posted: Thu Nov 16, 2017 7:44 pm
by NHMike
Big Jay wrote:Interesting paper. I was especially interested in the research into the length of the remaining rectal stump and the method of reconnection. Basically the more rectum the better with a minimum of 4cm for best results. Also some sort of reservoir, be it J-Pouch, or Side-End, is significantly better in both the short and long term than a straight connection.
I met w/ the surgeon last week it sounds like his plan is guaranteed to result in LARS.
My tumor has completely disappeared after radiation but, when it existed, it was at 9cm from the anal verge. Still the surgeon wants to cut out my entire rectum down to the dentate line. I pointed out that he probably could safely leave 4-5cm of rectum but he told me that it's hard to make that measurement during surgery. So it's easier for him cut everything out. When I objected he said "you won't miss those extra centimeters". According to this research I will certainly miss them.
He also insists that a straight connection is just the same as a pouch. Again, per this research, that isn't the case. Guess it's time to find a different surgeon.
Please keep us posted on what happens here.
Re: LAR Syndrome and laparoscopic surgery, new paper on origins
Posted: Thu Nov 16, 2017 8:13 pm
by susie0915
NHMike wrote:susie0915 wrote:I remember the surgeon told me during my consultation, that women are generally easier to operate on as they tend to have a wider pelvis. I ended up having open surgery 5 weeks later to take care of my blockage, and yes the recovery was tougher, but it was okay. So I have both laparoscopic scars and a vertical incision from above the belly button down to the pubic bone. I did get an infection in the incision that I had to pack with gauze a couple times a day, but it was not that bad. You sound like you are healing and recovering pretty well.
I grew up in pretty rough financial conditions and we often skipped meals so I was pretty skinny growing up which probably accounts for the narrow pelvis. It sounds like you had colon surgery which accounts for the differences in our cuts. Mine is horizontal, about five inches below the belly button and about five inches long. So I have to be very careful about any folding motions that stress that direction. I would think that a vertical cut would be more difficult for recovery because you have the folding issue as well as dealing with sideways stresses.
They put in one staple on the left, one in the belly button, one on the upper right and a drain in the lower right. The drain hole is already covered over with skin. There's still a bandage on top of the right one but that's because it's so close to the Ileostomy. There are no bandages on the left side anymore. Things are going well. Some minor aches here and there and I do tend to overdo things so some of those aches are my fault. But nothing bad enough to take pain medication of any kind. So far.
My original surgery was laparoscopic for rectal cancer, just 3 tiny little incisions can't hardly see scars. The surgery for the blockage was the vertical cut. It was definitely tougher.
Re: LAR Syndrome and laparoscopic surgery, new paper on origins
Posted: Thu Nov 16, 2017 8:20 pm
by susie0915
Big Jay wrote:Interesting paper. I was especially interested in the research into the length of the remaining rectal stump and the method of reconnection. Basically the more rectum the better with a minimum of 4cm for best results. Also some sort of reservoir, be it J-Pouch, or Side-End, is significantly better in both the short and long term than a straight connection.
I met w/ the surgeon last week it sounds like his plan is guaranteed to result in LARS.
My tumor has completely disappeared after radiation but, when it existed, it was at 9cm from the anal verge. Still the surgeon wants to cut out my entire rectum down to the dentate line. I pointed out that he probably could safely leave 4-5cm of rectum but he told me that it's hard to make that measurement during surgery. So it's easier for him cut everything out. When I objected he said "you won't miss those extra centimeters". According to this research I will certainly miss them.
He also insists that a straight connection is just the same as a pouch. Again, per this research, that isn't the case. Guess it's time to find a different surgeon.
I have read in other studies that the pouch may be better short term but long there is no difference. My tumor was about 5 cm up. My issue was frequent smaller bowel movements. You're not destined to get lars. Some do great. You may never be the same but it is manageable and there are many things you can do. I am leading a pretty normal life. Once you give it some time you will figure out what works. There are many on this forum that can give advice.
Re: LAR Syndrome and laparoscopic surgery, new paper on origins
Posted: Thu Nov 16, 2017 10:16 pm
by chrisca
Big Jay wrote:Interesting paper. I was especially interested in the research into the length of the remaining rectal stump and the method of reconnection. Basically the more rectum the better with a minimum of 4cm for best results. Also some sort of reservoir, be it J-Pouch, or Side-End, is significantly better in both the short and long term than a straight connection.
I met w/ the surgeon last week it sounds like his plan is guaranteed to result in LARS.
My tumor has completely disappeared after radiation but, when it existed, it was at 9cm from the anal verge. Still the surgeon wants to cut out my entire rectum down to the dentate line. I pointed out that he probably could safely leave 4-5cm of rectum but he told me that it's hard to make that measurement during surgery. So it's easier for him cut everything out. When I objected he said "you won't miss those extra centimeters". According to this research I will certainly miss them.
He also insists that a straight connection is just the same as a pouch. Again, per this research, that isn't the case. Guess it's time to find a different surgeon.
If you had a complete tumor response, it's also worth investigating the Habr-Gama "watch and wait" protocol. Knowing what I do now, I would have gone that route, but I don't think it was really known in the US surgical community when I had my resection.
-Chris.
Re: LAR Syndrome and laparoscopic surgery, new paper on origins
Posted: Thu Nov 16, 2017 10:39 pm
by Big Jay
I did do watch and wait. At my one year scope we (I saw we because I stay awake for the flex sig) saw that something wasn't right. There was more fleshiness.. nodularity in medical terms... next to the scar that hadn't been there before. Biopsy came back as cancer. So, time to go back to the original plan for the TME. If it's coming back on the surface it may be coming back deeper into the muscle wall.
Re: LAR Syndrome and laparoscopic surgery, new paper on origins
Posted: Fri Nov 17, 2017 2:12 am
by O Stoma Mia
Here's another paper on surgery-induced bowel problems. It's from research in Brazil. It's not about cancer and not about laparascopic surgery, per se, but it has some interesting findings.
One of my interests is in the amount of damage caused when using the linesr and circular staplers to form the anastomosis. These staplers can cause damage to the Internal Anal Sphincter when they are inserted through the anal canal.
http://www.scielo.br/scielo.php?script=sci_arttext&pid=S2237-93632011000300004
Re: LAR Syndrome and laparoscopic surgery, new paper on origins
Posted: Fri Nov 17, 2017 3:40 pm
by heiders33
I spoke with my colorectal surgeon today. He was unfamiliar with this study and asked me to send it to him, which I did. He said it was likely they did high litigation of the IMA during my surgery, but he doesn't remember for sure as it was a couple of months ago now. He did spare the sphincter, as the tumor was higher up in the rectum. He said that the nerves in the artery are so microscopic that you cannot tell during surgery whether you are disrupting them, but that it's low on the list of priorities for a curative surgery where the goal is to get clean margins. He was surprised when I told him that the study indicated that laparoscopic surgery could put you at higher risk for LARS; he said he thought it would be lower risk due to the better imaging, or at least the same risk as open surgery. However, he is going to read the study. Anyway, I left feeling not so reassured, but we will see what happens after reversal.
{kind=link}