Rectal cancer (Stage 3A) diagnosed late June 2017
Re: Rectal cancer (Stage 3A) diagnosed late June 2017
I don't own a robe so that would be a problem. Maybe a thin, long-sleeve shirt using the arms to tie around my waist or stomach? I suppose I could stop off at Marshalls tomorrow night to see if I can find one there (tomorrow night is scheduled with laundry and grocery shopping for the gum and Crystal Light or Gatorade). I can appreciate how much help is worth in a hospital visit going through this.
6/17: ER rectal bleeding; Colonoscopy
7/17: 3B rectal. T3N1bM0. 5.2 4.5 4.3 cm. Lymphs: 6 x 4 mm, 8 x 6, 5 x 5
7/17-9/17: Xeloda radiation
7/5: CEA 2.7; 8/16: 1.9; 11/30: 0.6; 12/20 1.4; 1/10 1.8; 1/31 2.2; 2/28 2.6; 4/10 2.8; 5/1 2.8; 5/29 3.2; 7/13 4.5; 8/9 2.8, 2/12 1.2
MSS, KRAS G12D
10/17: 2.7 2.2 1.6 cm (-90%). Lymphs: 3 x 3 mm (-62.5%), 4 x 3 (-75%), 5 x 3 (-40%). 5.1 CM from AV
10/17: LAR, Temp Ileostomy, Path Complete Response
CapeOx (8) 12/17-6/18
7/18: Reversal, Port Removal
2/19: Clean CT
7/17: 3B rectal. T3N1bM0. 5.2 4.5 4.3 cm. Lymphs: 6 x 4 mm, 8 x 6, 5 x 5
7/17-9/17: Xeloda radiation
7/5: CEA 2.7; 8/16: 1.9; 11/30: 0.6; 12/20 1.4; 1/10 1.8; 1/31 2.2; 2/28 2.6; 4/10 2.8; 5/1 2.8; 5/29 3.2; 7/13 4.5; 8/9 2.8, 2/12 1.2
MSS, KRAS G12D
10/17: 2.7 2.2 1.6 cm (-90%). Lymphs: 3 x 3 mm (-62.5%), 4 x 3 (-75%), 5 x 3 (-40%). 5.1 CM from AV
10/17: LAR, Temp Ileostomy, Path Complete Response
CapeOx (8) 12/17-6/18
7/18: Reversal, Port Removal
2/19: Clean CT
Re: Rectal cancer (Stage 3A) diagnosed late June 2017
I can't speak for anyone but myself but I wouldn't have cared two licks if my ass was sticking out of my gown despite my best efforts. I promise you the nurses would care even less. They wade through shit and puss and all sorts of other nastiness every day. A couple of ass cheeks ain't going to make a dent.
40 y/o male (now 46), kids 11 & 14.
Dx 3/16/17, rectal cancer s3,t3,n1,m0
PROSPCT trial (FOLFOX in lieu of chemorad)
FOLFOX 4/5/17 - 6/26/17
LAR 7/31/17, temp ileo
pathological complete response
Adjuvant chemo cancelled (IDEA Study)
Ileo reversed 9/25/17
NED
1 year scans - clear
2 year scans - clear
3 year scans - clear
4 year scans - clear
5 year scans - clear (considered cured)
Dx 3/16/17, rectal cancer s3,t3,n1,m0
PROSPCT trial (FOLFOX in lieu of chemorad)
FOLFOX 4/5/17 - 6/26/17
LAR 7/31/17, temp ileo
pathological complete response
Adjuvant chemo cancelled (IDEA Study)
Ileo reversed 9/25/17
NED
1 year scans - clear
2 year scans - clear
3 year scans - clear
4 year scans - clear
5 year scans - clear (considered cured)
-
O Stoma Mia

- Posts: 1709
- Joined: Sat Jun 22, 2013 6:29 am
- Location: On vacation. Off-line for now.
Incisional and parastomal hernias
.
Avoiding parastomal and incisional hernias after surgery
http://coloncancersupport.colonclub.com/viewtopic.php?f=1&t=50471&p=387550#p387550
Avoiding parastomal and incisional hernias after surgery
http://coloncancersupport.colonclub.com/viewtopic.php?f=1&t=50471&p=387550#p387550
Re: Rectal cancer (Stage 3A) diagnosed late June 2017
NHMike wrote:I don't own a robe so that would be a problem. Maybe a thin, long-sleeve shirt using the arms to tie around my waist or stomach? I suppose I could stop off at Marshalls tomorrow night to see if I can find one there (tomorrow night is scheduled with laundry and grocery shopping for the gum and Crystal Light or Gatorade). I can appreciate how much help is worth in a hospital visit going through this.
Just have them give you an extra gown to put on backwards.
Anne, 40
Stage IIIB Rectal Cancer
T3N1bM0
2/21/17 Dx, Age 39
2/21/17 CEA 0.9
3/23/17 - 5/2/17 Chemoradiation, 28 treatments
6/14/17 Robotic LAR w/temp loop ileostomy, ovaries & fallopian tubes removed, 2/21 lymph nodes positive
7/24/17 - 12/18/17 CapeOx, 6 Cycles
7/24/17 Dx w/ovarian cancer
9/6/17 CA 125 11.1
11/27/17 CEA 2.6
12/5/17 CT NED
12/13/17 CEA 2.9
1/11/18 CA 125 8.6
1/23/18 Reversal
3/21/18 CT enlarged thymus
4/6/18 PET NED
7/10/18 CT NED
7/11/18 CEA 2.6
9/18 Bilateral Prophylactic Mastectomy
Stage IIIB Rectal Cancer
T3N1bM0
2/21/17 Dx, Age 39
2/21/17 CEA 0.9
3/23/17 - 5/2/17 Chemoradiation, 28 treatments
6/14/17 Robotic LAR w/temp loop ileostomy, ovaries & fallopian tubes removed, 2/21 lymph nodes positive
7/24/17 - 12/18/17 CapeOx, 6 Cycles
7/24/17 Dx w/ovarian cancer
9/6/17 CA 125 11.1
11/27/17 CEA 2.6
12/5/17 CT NED
12/13/17 CEA 2.9
1/11/18 CA 125 8.6
1/23/18 Reversal
3/21/18 CT enlarged thymus
4/6/18 PET NED
7/10/18 CT NED
7/11/18 CEA 2.6
9/18 Bilateral Prophylactic Mastectomy
-
O Stoma Mia
- Posts: 1709
- Joined: Sat Jun 22, 2013 6:29 am
- Location: On vacation. Off-line for now.
Re: Rectal cancer (Stage 3A) diagnosed late June 2017
NHMike wrote:I was reading about the distance from the AV and the impact on reversal in another thread so I decided to look it up and it's 5.1 CM and I'm not too sure what that means but it's higher than some and lower than others.
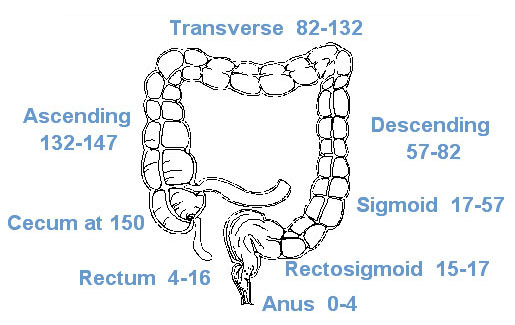
Ref: https://training.seer.cancer.gov/colorectal/anatomy/figure/figure1.html
My understanding of the anal verge is that this is the transition area where the mucus membrane of the anal canal meets the regular skin on the outside of the anus. Thus, the anal verge (AV) is at the very bottom of the anal canal. Above the AV you have about 4 cm of anal canal. Thus, if your report says that you have a 5.2 cm tumor that is 5.1 cm from the AV then this suggests that the lower part of the tumor is about 1.1 cm from the top of the anal canal, i.e., about a centimeter away from where the anal sphincters are located.
If one of the goals of the surgery is anal sphincter preservation, then the surgeon doesn't have much space to work with to remove the tumor with clear margins and still not cause any damage to the sphincters. I think this is why the treatment standard for rectal cancer is usually to have a series of neoadjuvant treatments prior to surgery in an attempt to shrink the tumor as much as possible and leave a cancer-free margin between the active tumor and the sphincters.
I also think that this is why they say that it is so important to have a Board Certified colorectal surgeon do the surgery.
Does this sound right?
Re: Rectal cancer (Stage 3A) diagnosed late June 2017
O Stoma Mia wrote:NHMike wrote:I was reading about the distance from the AV and the impact on reversal in another thread so I decided to look it up and it's 5.1 CM and I'm not too sure what that means but it's higher than some and lower than others.
Ref: https://training.seer.cancer.gov/colorectal/anatomy/figure/figure1.html
My understanding of the anal verge is that this is the transition area where the mucus membrane of the anal canal meets the regular skin on the outside of the anus. Thus, the anal verge (AV) is at the very bottom of the anal canal. Above the AV you have about 4 cm of anal canal. Thus, if your report says that you have a 5.2 cm tumor that is 5.1 cm from the AV then this suggests that the lower part of the tumor is about 1.1 cm from the top of the anal canal, i.e., about a centimeter away from where the anal sphincters are located.
If one of the goals of the surgery is anal sphincter preservation, then the surgeon doesn't have much space to work with to remove the tumor with clear margins and still not cause any damage to the sphincters. I think this is why the treatment standard for rectal cancer is usually to have a series of neoadjuvant treatments prior to surgery in an attempt to shrink the tumor as much as possible and leave a cancer-free margin between the active tumor and the sphincters.
I also think that this is why they say that it is so important to have a Board Certified colorectal surgeon do the surgery.
Does this sound right?
It sounds correct. So this is the answer to why they don't just go in and cut it out after diagnosis. I haven't paid close attention to things that aren't in the near-term but this is in the near-term for me now so I'm paying attention. From what I've read from others, my distance isn't great and it isn't bad. So we'll see how it goes. So yes, shrinking with chemorad is good.
Reading the article from Life Extension on the potential from metastasis from surgery was a little scary but it's an older article and I think that many of the recommendations are current practice today. There were two new forum member spouses with Mets after surgery (one was two months out and one a year out) and that's definitely scary stuff. You go through a difficult treatment protocol and then you're hit with Mets which is somewhat heartbreaking. I do think that you should go with the best specialists available to reduce the Metastasis risk going forward, in addition to improving the odds of some normalcy in living.
6/17: ER rectal bleeding; Colonoscopy
7/17: 3B rectal. T3N1bM0. 5.2 4.5 4.3 cm. Lymphs: 6 x 4 mm, 8 x 6, 5 x 5
7/17-9/17: Xeloda radiation
7/5: CEA 2.7; 8/16: 1.9; 11/30: 0.6; 12/20 1.4; 1/10 1.8; 1/31 2.2; 2/28 2.6; 4/10 2.8; 5/1 2.8; 5/29 3.2; 7/13 4.5; 8/9 2.8, 2/12 1.2
MSS, KRAS G12D
10/17: 2.7 2.2 1.6 cm (-90%). Lymphs: 3 x 3 mm (-62.5%), 4 x 3 (-75%), 5 x 3 (-40%). 5.1 CM from AV
10/17: LAR, Temp Ileostomy, Path Complete Response
CapeOx (8) 12/17-6/18
7/18: Reversal, Port Removal
2/19: Clean CT
7/17: 3B rectal. T3N1bM0. 5.2 4.5 4.3 cm. Lymphs: 6 x 4 mm, 8 x 6, 5 x 5
7/17-9/17: Xeloda radiation
7/5: CEA 2.7; 8/16: 1.9; 11/30: 0.6; 12/20 1.4; 1/10 1.8; 1/31 2.2; 2/28 2.6; 4/10 2.8; 5/1 2.8; 5/29 3.2; 7/13 4.5; 8/9 2.8, 2/12 1.2
MSS, KRAS G12D
10/17: 2.7 2.2 1.6 cm (-90%). Lymphs: 3 x 3 mm (-62.5%), 4 x 3 (-75%), 5 x 3 (-40%). 5.1 CM from AV
10/17: LAR, Temp Ileostomy, Path Complete Response
CapeOx (8) 12/17-6/18
7/18: Reversal, Port Removal
2/19: Clean CT
Re: Rectal cancer (Stage 3A) diagnosed late June 2017
re: robe: doubling up works well to cover the rear. One hospital robe facing front, another facing back
re: mets after surgery: that's why my husband took cimetidine and still takes it
Good luck!
re: mets after surgery: that's why my husband took cimetidine and still takes it
Good luck!
Wife 4/17 Dx age 45
5/17 LAR
Adenocarcinoma
low grade
1st primary T3 N2b M1a
Stage IVA
8/17 Sub-total colectomy
2nd primary 5.5 cm T1 N0
9 of 96 nodes
CEA: < 2.9
MSS
Lynch no; KRAS wild
Immunohistochemsistry Normal
Fall 2017 FOLFOX shrank the 1 met in liver
1/18 Liver left hepatectomy seg 4
5/18 CT clear
12/18 MRI 1 liver met
3/7/19 Resection & HAI
4/1/19 Folfiri & FUDR
5/13/19 HAI pump catheter dislodge, nearly bled to death
6-7 '19 5FU 4 cycles
NED
5/17 LAR
Adenocarcinoma
low grade
1st primary T3 N2b M1a
Stage IVA
8/17 Sub-total colectomy
2nd primary 5.5 cm T1 N0
9 of 96 nodes
CEA: < 2.9
MSS
Lynch no; KRAS wild
Immunohistochemsistry Normal
Fall 2017 FOLFOX shrank the 1 met in liver
1/18 Liver left hepatectomy seg 4
5/18 CT clear
12/18 MRI 1 liver met
3/7/19 Resection & HAI
4/1/19 Folfiri & FUDR
5/13/19 HAI pump catheter dislodge, nearly bled to death
6-7 '19 5FU 4 cycles
NED
Re: Rectal cancer (Stage 3A) diagnosed late June 2017
mpbser wrote:re: robe: doubling up works well to cover the rear. One hospital robe facing front, another facing back
re: mets after surgery: that's why my husband took cimetidine and still takes it
Good luck!
I have really big shoulders and doubling up doesn't work that well for me (I tried that when doing the MRIs). Maybe I should have received bigger sizes.
I know that there are folks here that push Cimetidine before surgery and I regret not asking my surgeon about it. I'll ask about it for afterwards though. I hope that your husband is doing well.
6/17: ER rectal bleeding; Colonoscopy
7/17: 3B rectal. T3N1bM0. 5.2 4.5 4.3 cm. Lymphs: 6 x 4 mm, 8 x 6, 5 x 5
7/17-9/17: Xeloda radiation
7/5: CEA 2.7; 8/16: 1.9; 11/30: 0.6; 12/20 1.4; 1/10 1.8; 1/31 2.2; 2/28 2.6; 4/10 2.8; 5/1 2.8; 5/29 3.2; 7/13 4.5; 8/9 2.8, 2/12 1.2
MSS, KRAS G12D
10/17: 2.7 2.2 1.6 cm (-90%). Lymphs: 3 x 3 mm (-62.5%), 4 x 3 (-75%), 5 x 3 (-40%). 5.1 CM from AV
10/17: LAR, Temp Ileostomy, Path Complete Response
CapeOx (8) 12/17-6/18
7/18: Reversal, Port Removal
2/19: Clean CT
7/17: 3B rectal. T3N1bM0. 5.2 4.5 4.3 cm. Lymphs: 6 x 4 mm, 8 x 6, 5 x 5
7/17-9/17: Xeloda radiation
7/5: CEA 2.7; 8/16: 1.9; 11/30: 0.6; 12/20 1.4; 1/10 1.8; 1/31 2.2; 2/28 2.6; 4/10 2.8; 5/1 2.8; 5/29 3.2; 7/13 4.5; 8/9 2.8, 2/12 1.2
MSS, KRAS G12D
10/17: 2.7 2.2 1.6 cm (-90%). Lymphs: 3 x 3 mm (-62.5%), 4 x 3 (-75%), 5 x 3 (-40%). 5.1 CM from AV
10/17: LAR, Temp Ileostomy, Path Complete Response
CapeOx (8) 12/17-6/18
7/18: Reversal, Port Removal
2/19: Clean CT
Re: Rectal cancer (Stage 3A) diagnosed late June 2017
NHMike wrote: . . . Maybe a thin, long-sleeve shirt using the arms to tie around my waist or stomach? . . .
That sounds like a PERFECT solution. When I had my 1st surgery, my brother was helping me walk those 1st few days. I was not allowed to walk by myself until 2 days out. I was not allowed to use a 2 gown (even with my hernia surgery). I was cut open, both surgeries .I was told I would only be allowed 1 gown because it is easier to get out of bed and move around in bed. Yes it hurt like h*ll getting out of bed each and every time. Maybe it's my short height, butt it was ALWAYS was a 2 person process to just get me to where my feet were over the bed.
I was not a big user of pain meds. I would not take it unless I needed to butt also STRESSED, if the staff asked I would take it. I pushed that pump 1x2 times EVERY time I got out of bed. For me it was worse than having to cough.
Maybe have something just in case.
Lee
rectal cancer - April 2004
46 yrs old at diagnoses
stage III C - 6/13 lymph positive
radiation - 6 weeks
surgery - August 2004/hernia repair 2014
permanent colostomy
chemo - FOLFOX
NED - 16 years and counting!
46 yrs old at diagnoses
stage III C - 6/13 lymph positive
radiation - 6 weeks
surgery - August 2004/hernia repair 2014
permanent colostomy
chemo - FOLFOX
NED - 16 years and counting!
Re: Rectal cancer (Stage 3A) diagnosed late June 2017
Lee wrote:NHMike wrote: . . . Maybe a thin, long-sleeve shirt using the arms to tie around my waist or stomach? . . .
That sounds like a PERFECT solution. When I had my 1st surgery, my brother was helping me walk those 1st few days. I was not allowed to walk by myself until 2 days out. I was not allowed to use a 2 gown (even with my hernia surgery). I was cut open, both surgeries .I was told I would only be allowed 1 gown because it is easier to get out of bed and move around in bed. Yes it hurt like h*ll getting out of bed each and every time. Maybe it's my short height, butt it was ALWAYS was a 2 person process to just get me to where my feet were over the bed.
I was not a big user of pain meds. I would not take it unless I needed to butt also STRESSED, if the staff asked I would take it. I pushed that pump 1x2 times EVERY time I got out of bed. For me it was worse than having to cough.
Maybe have something just in case.
Lee
Putting your arms through holes in the front seems fairly easy. Putting something like that on the back is harder as it's not designed for that and you need better range of motion and flexibility for that.
Almost done with my will and list of assets. I have to do another round of hibiclens, and do laundry for enough fresh clothes for tomorrow and Monday.
6/17: ER rectal bleeding; Colonoscopy
7/17: 3B rectal. T3N1bM0. 5.2 4.5 4.3 cm. Lymphs: 6 x 4 mm, 8 x 6, 5 x 5
7/17-9/17: Xeloda radiation
7/5: CEA 2.7; 8/16: 1.9; 11/30: 0.6; 12/20 1.4; 1/10 1.8; 1/31 2.2; 2/28 2.6; 4/10 2.8; 5/1 2.8; 5/29 3.2; 7/13 4.5; 8/9 2.8, 2/12 1.2
MSS, KRAS G12D
10/17: 2.7 2.2 1.6 cm (-90%). Lymphs: 3 x 3 mm (-62.5%), 4 x 3 (-75%), 5 x 3 (-40%). 5.1 CM from AV
10/17: LAR, Temp Ileostomy, Path Complete Response
CapeOx (8) 12/17-6/18
7/18: Reversal, Port Removal
2/19: Clean CT
7/17: 3B rectal. T3N1bM0. 5.2 4.5 4.3 cm. Lymphs: 6 x 4 mm, 8 x 6, 5 x 5
7/17-9/17: Xeloda radiation
7/5: CEA 2.7; 8/16: 1.9; 11/30: 0.6; 12/20 1.4; 1/10 1.8; 1/31 2.2; 2/28 2.6; 4/10 2.8; 5/1 2.8; 5/29 3.2; 7/13 4.5; 8/9 2.8, 2/12 1.2
MSS, KRAS G12D
10/17: 2.7 2.2 1.6 cm (-90%). Lymphs: 3 x 3 mm (-62.5%), 4 x 3 (-75%), 5 x 3 (-40%). 5.1 CM from AV
10/17: LAR, Temp Ileostomy, Path Complete Response
CapeOx (8) 12/17-6/18
7/18: Reversal, Port Removal
2/19: Clean CT
Re: Rectal cancer (Stage 3A) diagnosed late June 2017
NHMike wrote:Putting your arms through holes in the front seems fairly easy. Putting something like that on the back is harder as it's not designed for that and you need better range of motion and flexibility for that.
.
That makes sense to me. You've got me thinking about my surgery so many years ago. I had surgery on a Monday morning and was walking later that day. That 1st day, I walked twice, both times, 4 medical people were around me. I believe someone had a hold of me somehow both times. The next day, DB and a medical person for a good 1/2 day, I sent DB home to unwind and get good night sleep. A medical person walked with me the rest of the day. By the 3rd day, I was walking 10+ times a day. Sometimes BD or DH was walking with me, butt I was also walking by myself at this point. Someone always had to help me out of bed, butt after that I would walk, walk walk those halls. By Friday, I really just wanted to go home. I was hanging on the parking lot most of that day with regular clothes on. They sent me home Friday night. I suspect they were concern I would just up walk home.
Good luck, tomorrow, Monday and surgery,
Lee
rectal cancer - April 2004
46 yrs old at diagnoses
stage III C - 6/13 lymph positive
radiation - 6 weeks
surgery - August 2004/hernia repair 2014
permanent colostomy
chemo - FOLFOX
NED - 16 years and counting!
46 yrs old at diagnoses
stage III C - 6/13 lymph positive
radiation - 6 weeks
surgery - August 2004/hernia repair 2014
permanent colostomy
chemo - FOLFOX
NED - 16 years and counting!
Re: Rectal cancer (Stage 3A) diagnosed late June 2017
Mike:
I have not commented on your thread prior to this as I have not had anything to offer in the discussion.
But I do want to add another dose of well-wishes and prayer for your Monday surgery to those that have already been posted. Sending you added blessings and healing energy for a successful outcome.
If you need any ostomy pouching guidance or suggestions, I will be glad to offer - along with Lee and Aqx99. You have ostomy friends here, ready to extend a helping hand.
Karen
I have not commented on your thread prior to this as I have not had anything to offer in the discussion.
But I do want to add another dose of well-wishes and prayer for your Monday surgery to those that have already been posted. Sending you added blessings and healing energy for a successful outcome.
If you need any ostomy pouching guidance or suggestions, I will be glad to offer - along with Lee and Aqx99. You have ostomy friends here, ready to extend a helping hand.
Karen
Dear friend to Bella Piazza, former Colon Club member (NWGirl).
I have a permanent ileostomy and offer advice on living with an ostomy - in loving remembrance of Bella
I am on Palliative Care for broad endocrine failure + Addison's disease + osteonecrosis of both hips/jaw + immunosuppression. I live a simple life due to frail health.
I have a permanent ileostomy and offer advice on living with an ostomy - in loving remembrance of Bella
I am on Palliative Care for broad endocrine failure + Addison's disease + osteonecrosis of both hips/jaw + immunosuppression. I live a simple life due to frail health.
Re: Rectal cancer (Stage 3A) diagnosed late June 2017
YouTube video of the procedure: https://www.youtube.com/watch?v=iuUK7ucU98k
Pretty interesting that you can watch how the procedure should go along with the tools used. The tool for the video is a harmonic scalpel. It uses ultrasonic vibrations to simultaneously cut and cauterize tissue. The scalpel looks like a pair of jaws that come together on tissue. It can also be used to push tissue away as it's blunt instrument. You can see some smoke when the tissue is cut. There's also a stapling device but it seems to be used for multiple purposes: stapling, pushing things around. The overall process shows very little blood loss which is a good thing to reduce metastasis risk. The video is lap-assisted so it looks like the anus is open during the procedure. BTW, if you watch the video, you can see how delicate the whole thing is and it shows why you'd want a specialist for the procedure.
Thank-you for all of your prayers and well-wishes. They are most appreciated.
Pretty interesting that you can watch how the procedure should go along with the tools used. The tool for the video is a harmonic scalpel. It uses ultrasonic vibrations to simultaneously cut and cauterize tissue. The scalpel looks like a pair of jaws that come together on tissue. It can also be used to push tissue away as it's blunt instrument. You can see some smoke when the tissue is cut. There's also a stapling device but it seems to be used for multiple purposes: stapling, pushing things around. The overall process shows very little blood loss which is a good thing to reduce metastasis risk. The video is lap-assisted so it looks like the anus is open during the procedure. BTW, if you watch the video, you can see how delicate the whole thing is and it shows why you'd want a specialist for the procedure.
Thank-you for all of your prayers and well-wishes. They are most appreciated.
6/17: ER rectal bleeding; Colonoscopy
7/17: 3B rectal. T3N1bM0. 5.2 4.5 4.3 cm. Lymphs: 6 x 4 mm, 8 x 6, 5 x 5
7/17-9/17: Xeloda radiation
7/5: CEA 2.7; 8/16: 1.9; 11/30: 0.6; 12/20 1.4; 1/10 1.8; 1/31 2.2; 2/28 2.6; 4/10 2.8; 5/1 2.8; 5/29 3.2; 7/13 4.5; 8/9 2.8, 2/12 1.2
MSS, KRAS G12D
10/17: 2.7 2.2 1.6 cm (-90%). Lymphs: 3 x 3 mm (-62.5%), 4 x 3 (-75%), 5 x 3 (-40%). 5.1 CM from AV
10/17: LAR, Temp Ileostomy, Path Complete Response
CapeOx (8) 12/17-6/18
7/18: Reversal, Port Removal
2/19: Clean CT
7/17: 3B rectal. T3N1bM0. 5.2 4.5 4.3 cm. Lymphs: 6 x 4 mm, 8 x 6, 5 x 5
7/17-9/17: Xeloda radiation
7/5: CEA 2.7; 8/16: 1.9; 11/30: 0.6; 12/20 1.4; 1/10 1.8; 1/31 2.2; 2/28 2.6; 4/10 2.8; 5/1 2.8; 5/29 3.2; 7/13 4.5; 8/9 2.8, 2/12 1.2
MSS, KRAS G12D
10/17: 2.7 2.2 1.6 cm (-90%). Lymphs: 3 x 3 mm (-62.5%), 4 x 3 (-75%), 5 x 3 (-40%). 5.1 CM from AV
10/17: LAR, Temp Ileostomy, Path Complete Response
CapeOx (8) 12/17-6/18
7/18: Reversal, Port Removal
2/19: Clean CT
Re: Rectal cancer (Stage 3A) diagnosed late June 2017
Paper on a posterior approach from 2014 (with pictures):
https://bmcgastroenterol.biomedcentral. ... 30X-14-158
I guess that you can get an idea as to how difficult the surgery is from the paper and the pictures. The video view is with the camera with a mostly inside view. It doesn't show you how little space there is to work with.
"Low rectal cancer is a relatively common malignant disease with high morbidity and mortality rates [1, 2]. Globally, low anterior resection has been the mainstay of surgical therapy for rectal cancer since the 1970’s. Despite the best efforts of experienced surgeons, 5-year survival rates have ranged from 27% to 42% [3]. This conventional technique has also been associated with a high risk of damage to the autonomic pelvic nerve plexus, resulting in sexual and bladder dysfunction [3]."
Doing the MiraLax Prep now.
https://bmcgastroenterol.biomedcentral. ... 30X-14-158
I guess that you can get an idea as to how difficult the surgery is from the paper and the pictures. The video view is with the camera with a mostly inside view. It doesn't show you how little space there is to work with.
"Low rectal cancer is a relatively common malignant disease with high morbidity and mortality rates [1, 2]. Globally, low anterior resection has been the mainstay of surgical therapy for rectal cancer since the 1970’s. Despite the best efforts of experienced surgeons, 5-year survival rates have ranged from 27% to 42% [3]. This conventional technique has also been associated with a high risk of damage to the autonomic pelvic nerve plexus, resulting in sexual and bladder dysfunction [3]."
Doing the MiraLax Prep now.
6/17: ER rectal bleeding; Colonoscopy
7/17: 3B rectal. T3N1bM0. 5.2 4.5 4.3 cm. Lymphs: 6 x 4 mm, 8 x 6, 5 x 5
7/17-9/17: Xeloda radiation
7/5: CEA 2.7; 8/16: 1.9; 11/30: 0.6; 12/20 1.4; 1/10 1.8; 1/31 2.2; 2/28 2.6; 4/10 2.8; 5/1 2.8; 5/29 3.2; 7/13 4.5; 8/9 2.8, 2/12 1.2
MSS, KRAS G12D
10/17: 2.7 2.2 1.6 cm (-90%). Lymphs: 3 x 3 mm (-62.5%), 4 x 3 (-75%), 5 x 3 (-40%). 5.1 CM from AV
10/17: LAR, Temp Ileostomy, Path Complete Response
CapeOx (8) 12/17-6/18
7/18: Reversal, Port Removal
2/19: Clean CT
7/17: 3B rectal. T3N1bM0. 5.2 4.5 4.3 cm. Lymphs: 6 x 4 mm, 8 x 6, 5 x 5
7/17-9/17: Xeloda radiation
7/5: CEA 2.7; 8/16: 1.9; 11/30: 0.6; 12/20 1.4; 1/10 1.8; 1/31 2.2; 2/28 2.6; 4/10 2.8; 5/1 2.8; 5/29 3.2; 7/13 4.5; 8/9 2.8, 2/12 1.2
MSS, KRAS G12D
10/17: 2.7 2.2 1.6 cm (-90%). Lymphs: 3 x 3 mm (-62.5%), 4 x 3 (-75%), 5 x 3 (-40%). 5.1 CM from AV
10/17: LAR, Temp Ileostomy, Path Complete Response
CapeOx (8) 12/17-6/18
7/18: Reversal, Port Removal
2/19: Clean CT

Re: Rectal cancer (Stage 3A) diagnosed late June 2017
NHMike wrote:Paper on a posterior approach from 2014 (with pictures):
https://bmcgastroenterol.biomedcentral. ... 30X-14-158
I guess that you can get an idea as to how difficult the surgery is from the paper and the pictures. The video view is with the camera with a mostly inside view. It doesn't show you how little space there is to work with.
"Low rectal cancer is a relatively common malignant disease with high morbidity and mortality rates [1, 2]. Globally, low anterior resection has been the mainstay of surgical therapy for rectal cancer since the 1970’s. Despite the best efforts of experienced surgeons, 5-year survival rates have ranged from 27% to 42% [3]. This conventional technique has also been associated with a high risk of damage to the autonomic pelvic nerve plexus, resulting in sexual and bladder dysfunction [3]."
Doing the MiraLax Prep now.
Good luck, you've got this and stop reading stats!
I think you're more prepared than the average patient and certainly have done enough research to know what you're dealing with.
I admire your strength and understand the fears, but it's going to be okay
DX - 12/16
MSS - KRAS wild
Well-differentiated adenocarcinoma at splenic flexure
Stage IV CC with liver mets
5FU - Failed twice - 1/17 and 3/17
Irinotecan + Cetuximab: 8/17
Irinotecan and Erbitux ran it's course. CEA rising
Primary tumor invaded tail of pancreas and spleen. Liver mets major concern
Y-90 radioembolization on 9/17/18, liver enzyymes have dropped. 10 Radiation treatments to primary tumor completed too. CT scan Nov to assess overall situation...
MSS - KRAS wild
Well-differentiated adenocarcinoma at splenic flexure
Stage IV CC with liver mets
5FU - Failed twice - 1/17 and 3/17
Irinotecan + Cetuximab: 8/17
Irinotecan and Erbitux ran it's course. CEA rising
Primary tumor invaded tail of pancreas and spleen. Liver mets major concern
Y-90 radioembolization on 9/17/18, liver enzyymes have dropped. 10 Radiation treatments to primary tumor completed too. CT scan Nov to assess overall situation...
Return to “Colon Talk - Colon cancer (colorectal cancer) support forum”
Who is online
Users browsing this forum: Google [Bot] and 365 guests